
Peer Reviewed
New-Onset Ulcerative Colitis After Kidney Transplant Immunosuppression
Authors:
We’am Hussain, MD
Internal Medicine Resident, Wright State University, Dayton, Ohio
Drew Triplett, DO
Gastroenterology Fellow, Wright State University, Dayton, Ohio
Sangeeta Agrawal, MBBS
Professor of Internal Medicine; Gastroenterology Fellowship Director; Division Director, Gastroenterology, Wright State University, Dayton, Ohio
Citation:
Hussain W, Triplett D, Agrawal S. New-onset ulcerative colitis after kidney transplant immunosuppression. Consultant. 2020;60(3):95-96. doi:10.25270/con.2020.03.00009
A 60-year-old man presented to the emergency department with abdominal pain, mild rectal bleeding, tenesmus, and frequent liquid mucous stools for 18 days, reporting “loose stools” in the morning and several “explosive, watery stools” in the afternoon.
History. The man had a history of Alport syndrome for which he had undergone kidney transplant 12 years ago and for which he was taking tacrolimus and mycophenolic acid. He denied any gross blood in the stool, but guaiac fecal occult blood test results were positive, and he reported a 1.8-kg weight loss during his diarrheal illness. He had not undergone colonoscopy, and he reported no family history of inflammatory bowel disease (IBD).
Physical examination. His vital signs were within normal limits, and his body mass index was 24 kg/m2. Physical examination demonstrated general tenderness to deep palpation of the abdomen; the remainder of the physical examination findings were unremarkable.
Diagnostic tests. Results of routine laboratory studies were within normal limits, including a hemoglobin level of 15.3 g/dL, mean corpuscular volume of 87 µm3, and a white blood cell count of 8500/µL. Polymerase chain reaction test results for the toxin B gene of Clostridium difficile were negative. Stool cultures were negative for Salmonella, Shigella, Campylobacter, and Escherichia coli O157:H7. Results of a parasitology stool test were negative.
Inpatient colonoscopy was performed, during which erythema congestion and ulceration in the rectum, sigmoid colon, and descending colon were found (Figure 1). Biopsies were taken. On histological examination, the rectal, sigmoid, and descending colon mucosa showed mucosal hyperplasia with crypt abscess and evidence of acute and chronic inflammation (Figure 2). A diagnosis of ulcerative colitis (UC) was made.

Figure 1. A colonoscopy image suggested features of UC with erythema congestion and ulceration.
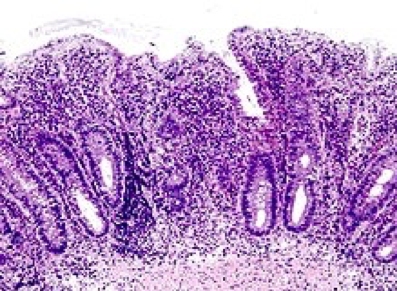
Figure 2. Histological examination showed mucosal hyperplasia with crypt abscess.
Treatment commenced with high-dose mesalamine, 1600 mg twice a day. His condition quickly improved; at 15 months’ follow-up, he continued to have no abdominal pain, and his bowel movements had returned to solid stools 3 times a day.
Discussion. After undergoing kidney transplant, patients commonly develop diarrhea due to infectious etiologies or due to the adverse effects of immunosuppressive medications. IBD such as UC is an uncommon cause of diarrhea after kidney transplant, particularly new-onset IBD.1 The presence of IBD is unexpected while patients are on immunosuppression, because IBD is believed to be the result of an inappropriately activated mucosal immune system, and immunosuppression is the treatment for IBD.1
This patient developed UC 12 years after his kidney transplant; this delay in presentation may have been the result of lesser use of corticosteroids in the late posttransplant period.2 Another explanation may be that the allograft may reconstitute a competent immune system in the recipient, and immunosuppressive therapy makes the patient susceptible to opportunistic infections that may trigger IBD manifestations.3 Moreover, tacrolimus is associated with a higher incidence of diarrhea. Tacrolimus inhibits peptidyl-prolyl isomerase enzyme activity and interferes with T-cell intracellular signaling.4 In some genetically predisposed individuals, tacrolimus may lead to the reduction of the CD8+ suppressor cells to a greater degree than other T-cell populations, increasing the helper-to-suppressor ratio; this T-cell imbalance has been reported to be an etiological factor in IBD.5
Therefore, although the development of IBD is rare after renal transplant, the effects of immunosuppressive medications and certain genetic predispositions may trigger an unusual presentation of IBD in an immunocompromised individual.
REFERENCES:
- Altıparmak MR, Trablus S, Pamuk ÖN, et al. Diarrhoea following renal transplantation. Clin Transplant. 2002;16(3):212-216.
- Riley TR, Schoen RE, Lee RG, Rakela J. A case series of transplant recipients who despite immunosuppression developed inflammatory bowel disease. Am J Gastroenterol. 1997;92(2):279-28
- Wahbeh G, Hupertz V, Hallowell S, Patel R, Chrisant MRK. Idiopathic colitis following cardiac transplantation: three pediatric cases. Pediatr Transplant. 2003;7(6):464-468.
- Sieber M, Baumgrass R. Novel inhibitors of the calcineurin/NFATc hub - alternatives to CsA and FK506? Cell Commun Signal. 2009;7:25.
- Matricon J, Barnich N, Ardid D. Immunopathogenesis of inflammatory bowel disease. Self Nonself. 2010;1(4):299-309.