
Peer Reviewed
Toxin-Mediated Erythema
Authors:
F. Hall Reynolds II, MD, MSc; Mark G. Tusa, MD; and Samuel L. Banks, MD
Chattanooga Skin and Cancer Clinic, Chattanooga, Tennessee
Citation:
Reynolds FH II, Tusa MG, Banks SL. Toxin-mediated erythema [published online June 11, 2018]. Consultant for Pediatricians.
Human illness due to protein toxin pose a formidable diagnostic dilemma. Increasing numbers of illnesses are being attributed to relate to toxins (bacterial or viral polypeptides) and relate to host susceptibility, microbial virulence, and perhaps new toxins being produced or identified. White and colleagues1 in 1989 introduced the concept that a protein toxin may function as a superantigen and activate excessive numbers of T lymphocytes. Since then, increasing numbers of illnesses have been attributed to toxins acting as superantigens. Clinical illnesses caused by streptococcal or staphylococcal toxins/superantigens may present similarly and are attributed to structural similarity of toxin molecules, with 3-dimensional structure being more important than amino acid sequence.2-5
Patients who present with erythema of both the perineal skin and the mucosa are a diagnostic challenge. Their skin abnormalities may represent an easily treated dermatitis or the early stages of a life-threatening illness. Clinical acumen is critical in solving the dilemma.
CASE REPORT
A 4-year-old boy had been in his usual state of good health until experiencing what had been considered to be a cold. Skin redness was noted in the distribution of his underwear, which prompted a visit to our general dermatology office a few days later. The redness had not caused itching or pain, nor had it interfered with bodily functions. There had been no systemic involvement such as fever, headache, loss of energy, irritability, or diarrhea.
History. His medications included montelukast and mometasone nasal spray for rhinitis, and amitriptyline-perphenazine for attention-deficit/hyperactivity disorder. There were no known medication allergies and no history of streptococcal infection, tonsillitis, or similar rash. His only history of skin disease was a localized infection with Hafnia alvei, a gastrointestinal tract commensal bacteria of the family Enterobacteriaceae that is usually pathogenic only with decreased immunity. This infection had been treated successfully 3 months before presentation with incision, drainage, and cephalexin.
Physical examination. Throughout the physical examination, the child was alert and active without distress. The conjunctivae appeared normal, but congestion and drainage of yellowish nasal mucus was conspicuous. His cheeks were flushed, his lips were cherry red, and his tongue was red with hypertrophied fungiform papillae (strawberry tongue) (Figure 1). The tonsils were minimally enlarged with mild erythema. Macular erythema with mild desquamation was present in the perineal skin, including the genital and perianal areas (Figures 2 and 3). No other skin abnormalities were noted, including on the hands, axillae, and feet. There was no peripheral edema and no enlargement of lymph nodes, liver, or spleen. The remainder of the examination findings were normal.

Figure 1. The patient’s cheeks were flushed, his lips were cherry red, and his tongue was red with hypertrophied fungiform papillae (strawberry tongue).

Figure 2. Macular erythema with mild desquamation was present in the perineal skin, including the genital area.

Figure 3. Macular erythema with mild desquamation was present in the perineal skin, including the perianal area.
Diagnosis. The most likely diagnosis was considered to be a streptococcal or staphylococcal infection of the upper respiratory tract, which was producing a toxin and provoking the clinical findings. Cultures were taken from the pharynx and the nose. Amoxicillin-clavulanate and prednisone were begun the same day by an otolaryngologist for associated otitis media.
Culture results of the tonsils and pharynx returned positive for group A Streptococcus pyogenes. Cultures of the nose grew normal flora of α-hemolytic streptococcus and Neisseria species. Toxin analysis was not performed by our laboratory.
Outcome of the case. Over the next 5 days, the patient was seen in the office twice more, and he remained healthy and playful. His upper respiratory tract infection resolved with antibiotic treatment, as did his rosy cheeks, cherry red lips, and strawberry tongue. The perineal skin erythema, which had involved his genitals, perianal area, and adjacent skin, progressively lightened and subsequently cleared with desquamation.
PATHOPHYSIOLOGY
Toxin-mediated erythema usually presents as a localized erythema of perineal skin and is mediated by a protein toxin, especially after streptococcal or staphylococcal pharyngitis. After infection, the organism manufactures and releases a polypeptide toxin into the bloodstream. If there is no protective antibody, the toxin circulates to the skin, where it functions, at least in part, as a superantigen.2,3,6
The typical immune response of a CD4 cell to a conventional protein antigen begins with phagocytosis of the antigen by an antigen-presenting cell (APC) such as a Langerhans cell or macrophage. The protein antigen is lysed into smaller peptides within the APC, which bind to the antigen groove of the major histocompatibility complex (MHC) class II molecules within the APC. This antigen peptide-MHC complex is then expressed on the surface of the APC. When the antigen and the MHC are recognized by all elements of a T-cell receptor (TCR) (Figure 4), the T cell is activated to proliferate clonally and release cytokines in a rather specific inflammatory response.2,6
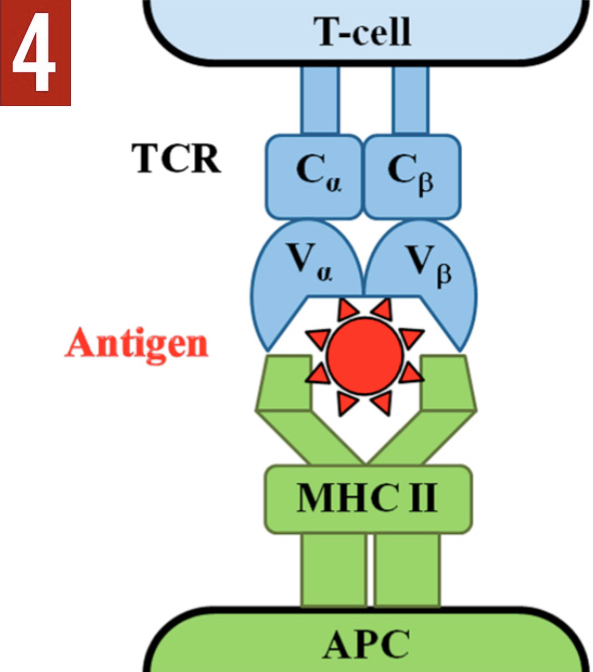
Figure 4. Conventional antigen processing. Reprinted with permission from: Macias ES, Pereira FA, Rietkerk W, Safai B. Superantigens in dermatology. J Am Acad Dermatol. 2011;64(3):455-472.6
A protein toxin that acts as a superantigen circumvents normal antigen processing (Figure 5). As an intact globular protein, a superantigen binds the MHC molecule of the APC directly to the Vβ element of the TCR. By direct cross-linking of the APC to the T-cell, a superantigen protein initiates an inflammatory cascade without phagocytosis by an APC, without breakdown into smaller peptides that are expressed in the antigen groove, and without recognition by all elements of the TCR.2,3,6-10 Only the Vβ chain of the TCR is required for recognition of a superantigen protein. This alternative mechanism allows a superantigen to initiate a nonspecific inflammatory process rather than a specific one. Massive clonal T-lymphocyte proliferation ensues, including CD4 and CD8 cells; polyclonal B-cell activation; profuse, unregulated proinflammatory cytokines (interferon-γ; tumor necrosis factor; interleukins 1,2, and 6; and others), additional chemical effectors, with resultant clinical manifestations such as fever, rash, hypotension, gastrointestinal tract symptoms, and other effects.2,3,6 In addition, a specific Vβ signature is produced, which allows for identification of the superantigen.6
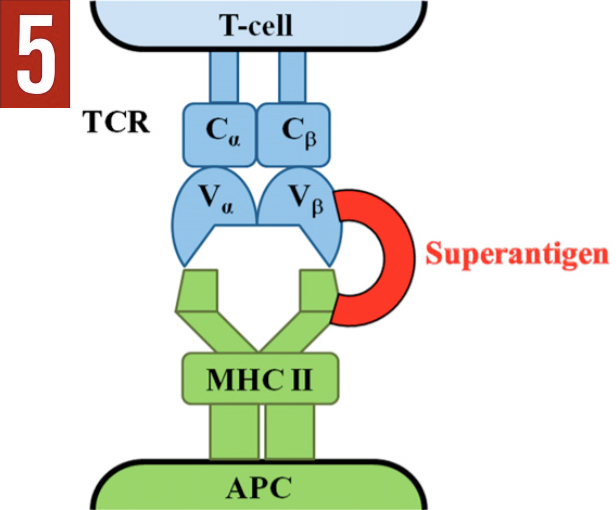
Figure 5. Superantigen direct activation. Reprinted with permission from: Macias ES, Pereira FA, Rietkerk W, Safai B. Superantigens in dermatology. J Am Acad Dermatol. 2011;64(3):455-472.6
It has been estimated that less than 1 T cell per 10,000 (0.01% to 0.1% of the body’s T-cells) responds when an antigen is processed in the conventional manner,10 but that superantigen T-cell activation may activate 5% to 30% of the entire T-cell population.2,4,6 Superantigens mainly activate CD4 cells but may activate any T cell with its 30,000 receptors, with approximately 100 of these receptors needed to recognize the antigen stimulus for clonal expansion to occur.6
DISCUSSION
Toxin-mediated erythema was recognized as a unique entity by Manders and colleagues in 1996.11 They described 2 patients with recurrent erysipelas-like perineal eruptions occurring shortly after nasopharyngeal bacterial infections, and they suggested that these cases represented a new variant of toxin-mediated disease. After distinguishing these cases from mucocutaneous lymph node syndrome (Kawasaki disease), they named the entity “recurrent toxin-mediated perineal erythema.” Toxins isolated in these 2 patients included streptococcal pyrogenic exotoxins A and B in the patient infected with group A β-hemolytic S pyogenes, and toxic shock syndrome (TSS) toxin 1 in the patient infected with methicillin-sensitive Staphylococcus aureus.
Two years later, Manders renamed the condition “toxin-mediated erythema” to accommodate clinical variations while still noting that most cases were recurrent and that there was a tendency for perineal involvement.2 This expanded insight included isolated episodes, recurrent erythroderma, and nondiagnostic presentations of TSS. The common feature among the clinical variants was the isolation of toxin-producing bacteria from sites that are normally sterile.
Clinical findings include pharyngitis caused by S pyogenes or, less likely, by S aureus.9,12 Other reported causes include impetigo and perianal cellulitis.3,6 Erythema develops within a few days—usually in the perineal region, including the genital and/or perianal areas, and adjacent skin—followed by resolution with desquamation, usually after appropriate therapy.
Additional findings may include cherry red lips, strawberry tongue, axillary erythema, and swelling with erythema of the hands and feet. Less common findings include perineal erythema and pustules,13 palmoplantar desquamation,3 and erythroderma and incomplete TSS.2 Toxin-mediated erythema typically occurs in young adults but has been reported in children as young as 2 years.3,13,14
Blood test results in Manders and colleagues’ original 2 cases revealed a mild leukocytosis but were otherwise negative, while skin biopsies revealed perivascular lymphohistiocytic infiltrates with sparse neutrophils.11 Patrizi and colleagues3 noted neutrophilic leukocytosis in 9 of their 11 pediatric cases, with normal platelet counts, erythrocyte sedimentation rates, and serum chemistry profiles. Patrizi and colleagues also obtained electrocardiograms and echocardiograms in 5 of their 11 patients and reported the results to be normal at 2 weeks after the onset of illness.
A superantigen toxin may also injure tissue apart from nonspecific inflammation, such as staphylococcal scalded skin syndrome (SSSS) in which staphylococcal exfoliative toxins A and B bind directly to transmembrane glycoprotein desmoglein 1 in the keratinocyte granular layer, causing lysis between keratinocytes.2,6,7,15-17 Desmoglein 1 is also the known autoantibody target in pemphigus foliaceus.15,16,18
Although the toxin in toxin-mediated erythema is considered to function as a superantigen, the illness it produces is clinically milder than other superantigen-mediated diseases. The patient may appear well. Mild fever or diarrhea may be present, but significant systemic toxicity is notably absent. Significant hypotension, organ dysfunction, or exceptional features should prompt a search for an alternative diagnosis. Interestingly, the anti-leukotriene effects of montelukast and the antihistamine effects of amitriptyline did not prevent the toxin from affecting our patient’s skin.
Other toxin-mediated superantigen illnesses that have been described include TSS (staphylococcal or streptococcal), recalcitrant erythematous desquamating disorder, scarlet fever, necrotizing fasciitis, and SSSS or its variant, staphylococcal scarlatiniform eruption.2,3,17 Potential superantigen toxin-mediated diseases include Kawasaki disease, psoriasis (guttate or plaque), atopic dermatitis, food poisoning, cutaneous T-cell lymphoma, sudden infant death syndrome, acute juvenile pityriasis rubra pilaris, and possibly others.2,6,7,10,13,17
The prognosis for toxin-mediated erythema is good. Prompt clearance is expected after appropriate antibiotic therapy but has been observed without therapy.3 Clinical sequelae also have been noted to occur despite antibiotic therapy.11 Recurrence is common, but our patient has remained healthy and without recurrence of nasopharyngeal infection or similar rash for more than 8 years. A broad differential diagnosis was considered in this patient and is presented in the accompanying Table.

REFERENCES
- White J, Herman A, Pullen AM, Kubo R, Kappler JW, Marrack P. The Vβ-specific superantigen staphylococcal enterotoxin B: stimulation of mature T cells and clonal deletion in neonatal mice. Cell. 1989;56(1):27-35.
- Manders SM. Toxin-mediated streptococcal and staphylococcal disease. J Am Acad Dermatol. 1998;39(3):383-398.
- Patrizi A, Raone B, Savoia F, Ricci G, Neri I. Recurrent toxin-mediated perineal erythema: eleven pediatric cases. Arch Dermatol. 2008;144(2):239-243.
- De Marzi MC, Fernández MM, Sundberg EJ, et al. Cloning, expression and interaction of human T-cell receptors with the bacterial superantigen SSA. Eur J Biochem. 2004;271(20):4075-4083.
- Schlievert PM, Bohach GA, Ohlendorf DH, et al. Molecular structure of staphylococcus and streptococcus superantigens. J Clin Immunol. 1995;15(6 suppl):4S-10S.
- Macias ES, Pereira FA, Rietkerk W, Safai B. Superantigens in dermatology. J Am Acad Dermatol. 2011;64(3):455-472.
- Ladhani S. Understanding the mechanism of action of the exfoliative toxins of Staphylococcus aureus. FEMS Immunol Med Microbiol. 2003;39(2):181-189.
- Skov L, Baadsgaard O. Superantigens: do they have a role in skin diseases? Arch Dermatol. 1995;131(7):829-832.
- Travers JB, Mousdicas N. Gram-positive infections associated with toxin production. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, eds. Fitzpatrick’s Dermatology in General Medicine. Vol 2. 8th ed. New York, NY: McGraw-Hill; 2012:2152-2159.
- Yarwood JM, Leung DYM, Schlievert PM. Evidence for the involvement of bacterial superantigens in psoriasis, atopic dermatitis, and Kawasaki syndrome. FEMS Microbiol Lett. 2000;192(1):1-7.
- Manders SM, Heymann WR, Atillasoy E, Kleeman J, Schlievert PM. Recurrent toxin-mediated perineal erythema. Arch Dermatol. 1996;132(1):57-60.
- Wojnarowska F, Cooper SM. Anogenital (non-venereal) disease. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 1. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2012:1171.
- Schoeffler A, Bollaert M, Muller P, Pouaha J, Werts F, Truchetet F. Recurrent toxin-mediated perineal erythema in an 11-year old child. Ann Dermatol Venereol. 2012;139:(6-7):477-480.
- El Bouch R, Reubsaet P, Koop K, Jansen J. A case of recurrent toxin-mediated perineal erythema. Arch Dis Child. 2013;98(10):776.
- Amagai M, Matsuyoshi N, Wang ZH, Andl C, Stanley JR. Toxin in bullous impetigo and staphylococcal scalded-skin syndrome targets desmoglein 1. Nat Med. 2000;6(11):1275-1277.
- Bukowski M, Wladyka B, Dubin G. Exfoliative Toxins of Staphylococcus aureus. Toxins. 2010;2(5):1148-1165.
- Solanki LS, Srivastava N, Singh S. Superantigens: a brief review with special emphasis on dermatologic diseases. Dermatol Online J. 2008;14(2):3.
- Wu H, Allan AE, Harrist TJ. Noninfectious vesiculobullous and vesiculopustular diseases. In: Elder DE, Elenitsas R, Rosenbach M, et al, eds. Lever’s Histopathology of the Skin. 11th ed. Philadelphia, PA: Wolters Kluwer; 2015:276-328.
- Darmstadt GL, Galen WK, Fischer G. Bacterial infections. In: Schachner L, Hansen RC, Happle R, et al, eds. Pediatric Dermatology. 3rd ed. Edinburgh, Scotland: Mosby; 2003:998-999.
- Marks VJ, Maksimak M. Perianal streptococcal cellulitis. J Am Acad Dermatol. 1988;18(3):587-588.
- Herbst, RA. Perineal streptococcal dermatitis/disease: recognition and management. Am J Clin Dermatol. 2003;4(8):555-560.
- Parsons ME, Ray MC, Rietschel RL. Episodic nontoxic erythema. Arch Dermatol. 1996;132(11):1387-1388.
- Beltraminelli H, Itin P. Erythema scarlatiniforme desquamativum recidivans—a forgotten disease (recurring localized scarlatiniform scaled erythema). Dermatology. 2006;212(3):211-213.
- Braun-Falco M, Kasche A, Worret WI. Recurring localized scarlatiniform scaled erythema of Féréol-Besnier. Dermatology. 2006;212(3):253-257.
ACKNOWLEDGEMENT
The authors acknowledge Philip J. Andrews, NP, for technical assistance in preparing the original manuscript.