
Pearls of Wisdom: Vitamin Supplementation in Smokers
Jack is a 62-year-old committed smoker. He has coronary artery disease, chronic obstructive pulmonary disease, and heart failure, and was recently taken off the heart transplant list when it was discovered that he was still smoking. At a recent trip to the health food store, he returned with vitamin E and beta carotene supplements that had been recommended by the store clerk, who suggested that their antioxidant activity would help prevent lung cancer.
What would you tell your patient?
A. Studies have shown that antioxidant vitamins reduce the incidence of lung cancer by as much as 20%.
B. Studies have shown that antioxidant vitamins only reduce lung cancer by about 5%, so decisions must be individualized.
C. Studies have shown that antioxidant vitamins are neutral in respect to lung cancer.
D. Studies have shown that antioxidant vitamins worsen outcome in respect to lung cancer.
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Smokers should avoid beta carotene supplementation.
The billions of dollars spent on vitamins and supplements each year in the United States is by no means a result of activity on the part of physicians or public health officials. Most clinicians are aware that if there is any benefit to the long-term administration of multivitamins or individual components to otherwise healthy individuals, it must be very small, because clinical trial data have a difficult time confirming such positive outcomes. Why a long-term smoker would spend time, effort, and money to find a deterrent to lung cancer rather than stopping smoking might seem mysterious—except that it is not an uncommon story.
_________________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Can TMS Aid Smoking Cessation Efforts?
Could Metabolism Affect Smoking Cessation Efforts?
_________________________________________________________________________________________________________________________________________________________________________
Patients get their medical information from diverse sources, with equally diverse veracity to the information they receive. Patients may or may not be in a position to judge the capacity of the person providing medical advice. Advertising has capitalized upon the appeal of terminologies that have allure based upon their simplistic syllogistic thinking: oxidation is bad > antioxidants prevent oxidation > antioxidants must be a really good thing.
Research
Our consideration of antioxidants for lung cancer prevention came along through a scientifically respectable pathway: observational data. Recall that observational data, no matter how compelling, can only be considered hypothesis-generating: Observational data can identify association but not establish causation.
Observational data had shown that the folks who consumed the most beta carotene and vitamin E had the lowest rates of lung cancer. It didn’t take but a small leap from there to decide: well, let’s try it.
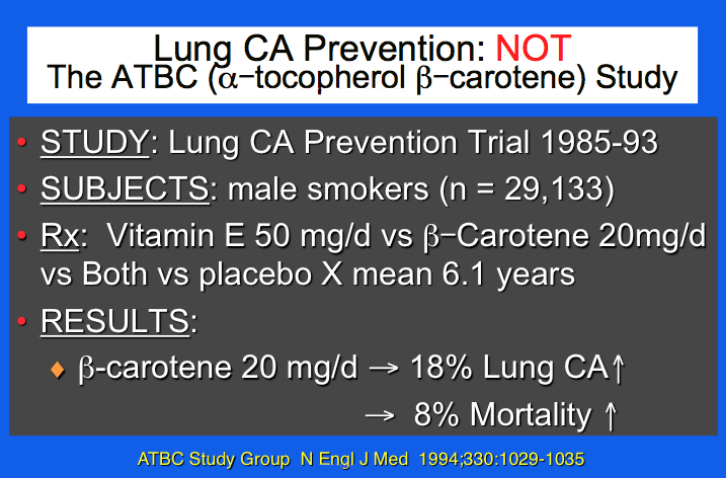
In the Alpha-Tocopherol Beta Carotene Cancer Prevention (ATBC) Study,1 a large population of male smokers (N = 29,133) were invited to participate in a placebo-controlled trial comparing vitamin E and beta carotene. At the 6-year conclusion of the trial, an 18% increase in lung cancer and an 8% increase in mortality were noted.

Apparently undaunted by these negative results, the beta-Carotene and Retinol Efficacy Trial (CARET)2 featured a similarly large population (N = 18,314) of men and women, this time including more than 4000 asbestos workers—surely a very high-risk group. Originally scheduled to go on for 6 years, the trial was terminated early because of a 28% increase in lung cancer and 17% increase in mortality.
Much of the time, clinicians opt for a “benign neglect” approach to patients who query the propriety of vitamin supplements. At least in the case of beta carotene for persons at risk for lung cancer, the ATBC Study got it right: Smokers should avoid beta carotene supplementation.3
What’s the “Take Home”?
For smokers, smoking cessation is the best way to reduce risk for lung cancer. Although lung cancer screening has recently been endorsed by major guidance agencies (eg, the US Preventive Services Task Force), no intervention surpasses the efficacy of smoking cessation for reducing the risk of lung cancer and cardiovascular disease. Well-intended but misguided steps that appear innocuous may not be so—beta carotene in smokers is a good example.
References:
1. Alpha-Tocopherol Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med. 1994;330(15):1029-1035.
2. Omenn GS, Goodman G, Thornquist M, et al. Chemoprevention of lung cancer: the beta-Carotene and Retinol Efficacy Trial (CARET) in high-risk smokers and asbestos-exposed workers. IARC Sci Publ. 1996;(136):67-85.
3. Virtamo J, Pietinen P, Huttunen JK, et al; ATBC Study Group. Incidence of cancer and mortality following α-tocopherol and β-carotene supplementation: a postintervention follow-up. JAMA. 2003;290(4):476-485.