
Peer Reviewed
Solitary Rectal Ulcer Syndrome With Polyposis
Authors:
Meghana Nadiger, MD
Department of Pediatrics, Flushing Hospital Medical Center, Queens, New York
Maximillian A. Weigelt
Medical Student, American University of the Caribbean, Pembroke Pines, Florida
Susana Rapaport, MD
Department of Pediatrics, Flushing Hospital Medical Center, Queens, New York
Babu S. Bangaru, MD
Chief, Division of Pediatric Gastroenterology, Flushing Hospital Medical Center, Queens, New York; Clinical Associate Professor, Department of Pediatrics, New York University School of Medicine, New York, New York
Citation:
Nadiger M, Weigelt MA, Rapaport S, Bangaru BS. Solitary rectal ulcer syndrome with polyposis [published online November 12, 2018]. Gastroenterology Consultant.
A 14-year-old boy presented with a 2-week history of diarrhea with bright red rectal bleeding. He had had intermittent diarrhea with bleeding for more than 2 years.
History. He denied having abdominal pain, constipation, straining, or pain during defecation. There were no intestinal or extraintestinal manifestations of inflammatory bowel disease (IBD). There was no history suggestive of bleeding problems or clotting problems. He was a known patient with a diagnosis of thalassemia minor. There was no history of drug use or sexual activity. Family history was significant for a sister who had undergone colectomy for ulcerative colitis.
The boy had been seen 2 years ago with a 2-month history of diarrhea with bright rectal bleeding, weight loss of 3.2 kg, and arthralgias, the latter of which had been diagnosed as “growing pains.” There was no other significant medical history. At that time, a complete blood cell count (CBC) showed changes consistent with his thalassemia minor but was otherwise normal. Comprehensive metabolic panel (CMP) results, erythrocyte sedimentation rate, C-reactive protein level, celiac disease antibody panel results, thyroid function test results, stool calprotectin level, stool culture results, Entamoeba histolytica antigen, and Clostridium difficile toxins A and B were all normal or negative. Coagulation studies showed mild von Willebrand disease, which was felt to be not clinically significant. Colonoscopy with terminal ileal intubation and magnetic resonance enterography showed no evidence of IBD. He had been lost to follow-up.
Physical examination. At the current presentation, the boy’s vital signs were stable. Height, weight, and body mass index were normal. There was no scleral icterus or uveitis. There were no aphthous ulcers. The abdomen was soft and nontender with no organomegaly. There were no perianal lesions. The remainder of the physical examination findings were normal. Rectal examination revealed an empty ampulla and yielded no stool for guaiac testing.
Diagnostic tests. Laboratory test results were again unremarkable, with CBC, CMP, inflammatory markers, iron panel, and stool calprotectin all within normal limits. Results of stool studies for E histolytica and C difficile antigens were negative.
Colonoscopy was done, the results of which showed that changes were limited to the rectum (Figure 1). The rest of the colon and the terminal ileum were normal.
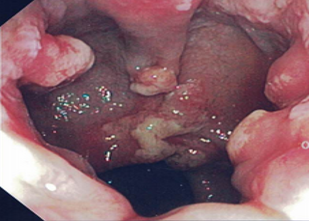

Figure 1. Colonoscopy findings at presentation showing multiple polypoidal lesions with whitish gray exudate covering the apical portions of the polyps, with surrounding erythema and friability.
Rectal biopsy showed ulcerated rectal mucosa with acute inflammatory exudate, granulation tissue formation, villous transformation of mucosa, and fibromuscular proliferation in the lamina propria. Based on these results, solitary rectal ulcer syndrome (SRUS) with polyposis was diagnosed.
The findings from the boy’s visit 2 years ago were reviewed. On colonoscopy, a thickened appearance of the mucosa of the anterior rectal wall was noted. Rectal biopsies showed mild glandular and smooth muscle hyperplasia, consistent with prolapse change (Figure 2). Biopsies from the other areas of the colon and the ileum were normal.
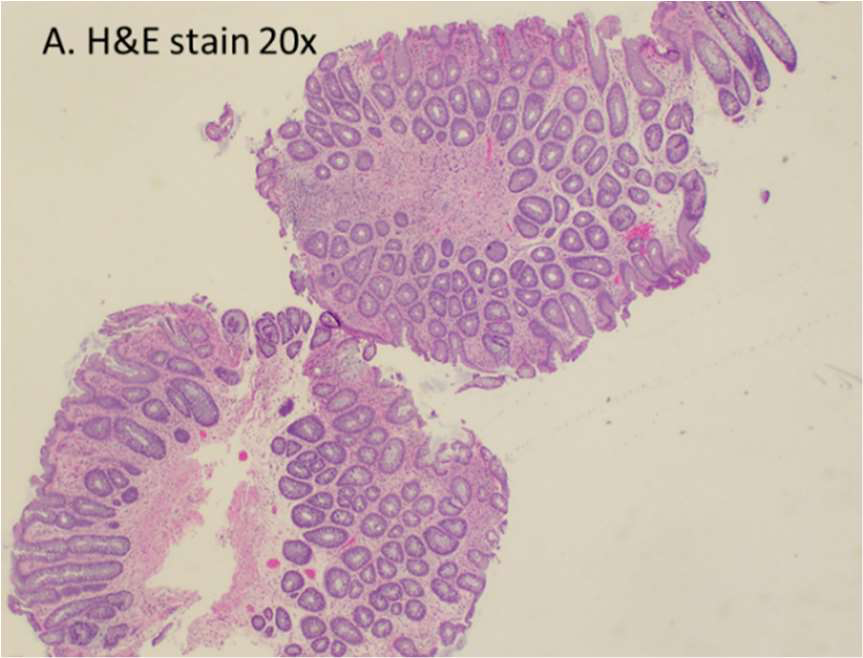
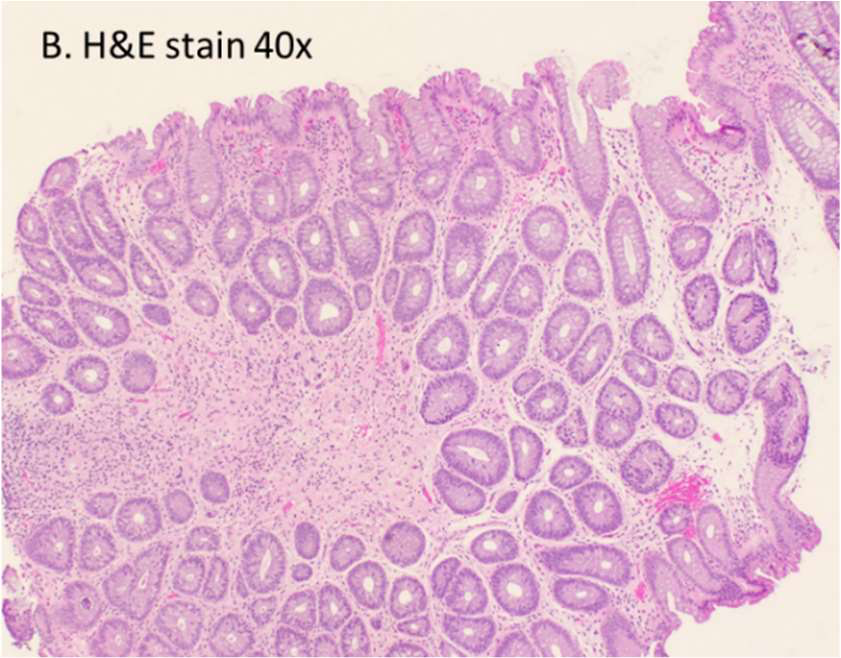
Figure 2. Photomicrographs of rectal biopsy showing shows colonic type mucosa with mild glandular and smooth muscle hyperplasia, consistent with prolapse change. There is no dysplasia or inflammation.
Discussion. SRUS is a rare, benign disorder of the rectum and sigmoid colon, with an estimated worldwide annual incidence of 1 in 100,000.1 It mainly affects young adults, although a few case series and cases have been described in children and in the geriatric population.
SRUS was first described in 1829, and the term solitary ulcers of the rectum was used in the 1930s. The name is now a misnomer. The possible range of rectal lesions includes hyperemic mucosa, single or multiple ulcers, and single or multiple polyps or polypoid lesions, with solitary ulcers described in only about 20% of cases.2 Common presenting symptoms include rectal bleeding, passage of mucus, straining on defecation, tenesmus, and perineal and abdominal pain. Other reported symptoms include diarrhea, sensation of incomplete defecation, constipation, feeling of incomplete defecation, and self-digitation.3
The pathogenesis is unclear.3,4 One theory suggests that prolapse of the rectal mucosa secondary to excessive straining is an important factor.4 High intrarectal pressure forces the anterior rectal mucosa against the contracting puborectalis muscle, often into the anal canal, resulting in congestion, edema, pressure necrosis, and ulceration.4 Direct mucosal trauma, rectal dysmotility, and ischemia seem to play a part. It appears to be part of pelvic floor dysfunction syndrome.
Colonoscopic lesions consisting of focal hyperemia, thickened mucosal appearance, one or more ulcers, and polypoidal lesions limited to the rectum (and, at times, the lower sigmoid colon), more likely in the anterior rectum, should raise the suspicion of the diagnosis of SRUS. The diagnosis is established by the characteristic histologic finding of fibromuscular obliteration of the lamina propria.1,4,5,6 Hyperplastic or serrated changes of crypt architecture and thickening of the muscularis mucosae are often noted.4,5
SRUS is exceedingly rare in children, with few case reports having been published7; the 3 largest pediatric case series comprised 22, 55, and 31 patients, respectively.6-8 Anemia, decreased appetite, and poor weight gain/growth have been described.9 The clinical variability of SRUS may cause it to be mistaken for other diseases such as IBD, infectious proctocolitis, intussusception, hemorrhoids, and juvenile polyps.4 Polypoid variants may be mistaken for malignancy. This combination of rarity, a low index of suspicion, and clinical variability often leads to delayed diagnosis or misdiagnosis. As such, even in the absence of symptoms, diagnosis requires a full ileocolonoscopy with multiple biopsies.8
The optimal treatment of SRUS has not been clearly established and must be individualized. Regulation of stooling habits, avoiding excessive straining and self-digitation, judicious use of stool softeners, and a high-fiber diet appear to be of paramount importance.4 Behavioral and psychosocial issues need to be explored. Options reported in the literature include anti-inflammatory agents in the form of enemas (sucralfate, salicylates, sulfasalazine, and steroids), behavior modification, biofeedback, botulinum toxin injection, and rectopexy. Full recovery has been reported in up to 70% of patients with proper management.6
Outcome of the case. In our patient, further questioning revealed that he had been observed to spend a lot of time on the toilet. He admitted to self-digitation and straining. He was hesitant to admit these symptoms. He was counseled and was put on high-fiber diet and a daily bedtime dose of mineral oil. At follow-up 1 year later, he reported marked improvement. He noted that he usually has 1 soft bowel movement daily, and that he occasionally notices blood in small amounts. He claims to no longer need to strain and to have stopped self-digitation. Colonoscopy showed marked improvement, with only one polypoidal lesion noted in the anterior rectum (Figure 3).

Figure 3. A recent colonoscopy image showing only 1 lesion, and the others healed.
- Saadah OI, Al-Hubayshi MS, Ghanem AT. Solitary rectal ulcer syndrome presenting as polypoid mass lesions in a young girl. World J Gastrointest Oncol. 2010;2(8):332-334.
- Zhu Q-C, Shen R-R, Qin H-L, Wang Y. Solitary rectal ulcer syndrome: clinical features, pathophysiology, diagnosis and treatment strategies. World J Gastroenterol. 2014;20(3):738-744.
- Keshtgar AS. Solitary rectal ulcer syndrome in children. Eur J Gastroenterol Hepatol. 2008;20(2):89-92.
- Abreu M, Azevedo Alves R, Pinto J, Campos M, Aroso S. Solitary rectal ulcer syndrome: a paediatric case report. GE Port J Gastroenterol. 2017;24(3):142-146.
- Perito ER, Mileti E, Dalal DH, et al. Solitary rectal ulcer syndrome in children and adolescents. J Pediatr Gastroenterol Nutr. 2012;54(2):266-270.
- Dehghani SM, Bahmanyar M, Geramizadeh B, Alizadeh A, Haghighat M. Solitary rectal ulcer syndrome: is it really a rare condition in children? World J Clin Pediatr. 2016;5(3):343-348.
- Suresh N, Ganesh R, Sathiyasekaran M. Solitary rectal ulcer syndrome: a case series. Indian Pediatr. 2010;47(12):1059-1061.
- Kowalska-Duplaga K, Lazowska-Przeorek I, Karolewska-Bochenek K, et al. Solitary rectal ulcer syndrome in children: a case series study. Adv Exp Med Biol. 2017;1020:105-112.
- Madigan MR, Morson BC. Solitary ulcer of the rectum. Gut. 1969;10(11):871-881.