
Soccer Accident Results in Severe Knee Pain
 |  |  |
A 23-year-old woman presents with severe right knee pain that resulted from a collision with another player during a soccer game. The majority of the force of the blow was to the right knee. The medical history is noncontributory.
This thin, athletic woman is in moderate distress because of her knee pain. Temperature is 37.2oC (99oF); heart rate, 72 beats per minute with normal rhythm; respiration rate, 15 breaths per minute; and blood pressure, 108/74 mm Hg. Head and neck are normal, lungs are clear, and upper extremities and left lower extremity are normal. Sensation in the right foot and area about the knee is intact. Pulses in the right groin, popliteal region, and right foot are normal. The area about the right knee joint is moderately swollen—particularly laterally; in addition, the joint appears deformed. Severe pain limits passive and active motion of the knee.
You order frontal, lateral, and sunrise radiographs of the right knee. What do these films reveal about the extent of this patient’s injury?
 |  |  |
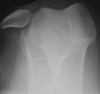
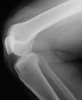
Knee pain following a soccer injury: The frontal radiograph reveals that the patella is dislocated laterally (A). This is confirmed on the sunrise radiograph (B). A lateral radiograph shows the malalignment of the patella with the distal femur (C). Most important, it also shows no fracture. Lateral dislocation of the patella is diagnosed.
Factors that predispose to patellar dislocations include:
- Shallow trochlear groove.
- Shallow posterior patellar margin.
- Ligamentous laxity (associated with several conditions, such as Marfan syndrome or Ehlers-Danlos syndrome).


In the vast majority of patients, the initial patellar dislocation represents injury to the medial patellar femoral ligament. Such an injury increases a patient’s risk of subsequent dislocations. The medial patellar femoral ligament originates at the medial epicondyle and inserts at the superior margin of the medial aspect of the patella. The primary function of the ligament is to resist lateral migration of the patella. In most patients, when the ligament is disrupted, it has been avulsed from the medial epicondyle. Avulsion fractures in the medial epicondyle may be associated with this type of injury.
Therapy for an initial dislocation is typically nonoperative unless a definite chondral injury or fracture is identified. Reduce the dislocation by applying medial pressure to the patella, with the hip in flexion and the knee extended. It is recommended that reduction be followed by a period of immobilization to allow the medial retinaculum to repair itself. Immobilization is followed by rehabilitation aimed at strengthening the quadriceps musculature to help maintain stability. There is a high risk of recurrence in up to 50% of patients.
Surgical management typically involves inspection and repair of the medial patellar femoral ligament. MRI may be helpful preoperatively to identify the location and degree of injury.
Outcome of this case. The patient’s dislocation was reduced externally. A frontal radiograph of the knee obtained after the reduction shows normal alignment of the patella and the distal femur (D). This is confirmed by a post-reduction lateral view (E). At 3 months, the patient has not had a recurrence.