
Mind the Gap: Strategies to Improve Communication Between Clinical and Nonclinical Audiences Around AAD Symptom Recognition and Diagnosis
Disclosures of support:
Otsuka America Pharmaceutical, Inc. funded a series of discussion panels for experts in the AAD space as well as the participation in writing this expert opinion paper. JC is supported by NIGMS grant P20GM109025; NINDS grant U01NS093334; NIA grant R01AG053798; NIA grant P20AG068053; NIA grant P30AG072959; NIA grant R35AG71476; Alzheimer’s Disease Drug Discovery Foundation (ADDF); Ted and Maria Quirk Endowment; and the Joy Chambers-Grundy Endowment.
Conflict of interest statement:
JC has provided paid consultation to Acadia, Karuna, Lundbeck, Suven, and Otsuka America Pharmaceutical, Inc. ST has provided paid consultation to Eisai, USAgainstAlzheimers, Gates Ventures, Lilly, Biogen and Otsuka America Pharmaceutical, Inc. Other authors declare no conflict of interest.
Abstract
Agitation in Alzheimer’s dementia is a serious neuropsychiatric condition that is highly prevalent and underdiagnosed. It contributes to adverse clinical outcomes for people living with Alzheimer’s dementia and causes significant burden for care partners. In response to evidence of miscommunication from a social listening analysis, the Global Council on Alzheimer’s Disease (GCAD) collaborated with Otsuka Pharmaceutical Development & Commercialization, Inc., to sponsor a series of three virtual agitation in Alzheimer’s dementia expert panels involving both healthcare professionals and people who have lived experience with agitation in Alzheimer’s dementia. The panels were held from February-August 2022 to gain insights and address challenges concerning lexicon differences among stakeholders, symptom recognition, and the lack of clarity regarding the definition and description of agitation in Alzheimer’s dementia. This report will summarize the agitation in Alzheimer’s dementia expert panel series key findings, provide an expert perspective on the current agitation in Alzheimer’s dementia landscape, identify challenges to recognition and diagnosis (including communication barriers), and discuss strategies to improve the conversation around agitation in Alzheimer’s dementia.
Introduction
Alzheimer’s disease (AD) is a highly prevalent neurodegenerative disorder. Most individuals with AD will experience neuropsychiatric symptoms (NPS), such as agitation in Alzheimer’s dementia (AAD). AAD can seriously impact the health and quality of life of both the person living with AAD and those providing care for them.1-3 However, mental health problems in older populations tend to be under-recognized by both the elderly persons and their care providers.4 Claim-based studies have shown evidence for AAD underdiagnosis, with only a small percentage of patients who exhibited symptoms of agitation receiving a diagnosis for it.5
In research contracted by Otsuka, a lexicon analysis of social listening research evaluating data from online communication forums collected from April 2020 to May 2021, it was found that there is a divergence in the use of the term “agitation” between clinical and nonclinical stakeholders. Care partners more frequently used agitation colloquially, as an adjective to describe behavior and reactions more generally, while healthcare professionals and professional organizations used agitation as a clinical term, as it connected to dementia and AD. Care partners are a key source of information during the diagnostic process, often taking on roles such as communicating and coordinating care with other family members and healthcare providers.6 However, care partners are vulnerable to the mental and emotional challenges that come with supporting a person living with AAD, which can impact symptom recognition and reporting; incorrect or incomplete reporting by care partners can result in underdiagnosis of AAD.7
Otsuka convened three multidisciplinary expert panels from February-August 2022. They consisted of fourteen experts from multiple disciplines spanning clinical practice, social work, research, advocacy, care partners, and people living with AAD. The purpose of the panels was to further explore gaps in communication and identify strategies to improve treatment and diagnosis of AAD.
More specifically, the goals of the AAD expert panels were to:
- Gain insights from advocates, people living with AAD, care partners, and professionals whose work or experience involves AAD, and
- Discuss how to improve the process of AAD diagnosis by aligning on clear and easily comprehended language to increase understanding and recognition of AAD symptoms in communications between clinical and nonclinical stakeholders.
We provide an overview of AD and AAD, followed by a summary of the key takeaways of the panels on identification and discussion of AD, a description of nonpharmacologic management options for AAD, and a discussion on the evolving landscape of AAD pharmacologic treatment.
Overview of Agitation in Alzheimer’s Dementia (AAD)
Alzheimer’s disease is the most common form of dementia.6 In 2024, there were an estimated 6.9 million adults aged ≥65 years living with AD in the United States; this population is projected to reach 12.7 million by 2050.6 Most individuals with AD dementia are cared for in the home, as an estimated 65% of US adults with AD dementia and other forms of dementia lived in the community in 2024, requiring more care from family members and other unpaid care partners as their disease progressed.6 Despite its prevalence, dementia is under-recognized; according to research conducted on the National Health and Aging Trends Study data, 39.5% of patients with probable dementia were undiagnosed.8
The continuum of AD progression includes six phases according to the FDA staging system (Figure 1). There are two preclinical stages: Stage 1, in which the patient may have abnormal biomarkers, but no detectable symptoms, and Stage 2, where the patient may experience subtle cognitive effects, but no functional deficits. Stage 3 is mild cognitive impairment (MCI) due to AD, where symptoms are mild and do not interfere with everyday activities. Stages 4 through 6 are categorized as dementia due to AD, progressing from mild, moderate, to severe symptoms that interfere with daily activities of life.6,9 However, this seamless progression through the continuum is not universally experienced by all patients; not everyone with MCI due to AD progresses to AD dementia at the same rate.6
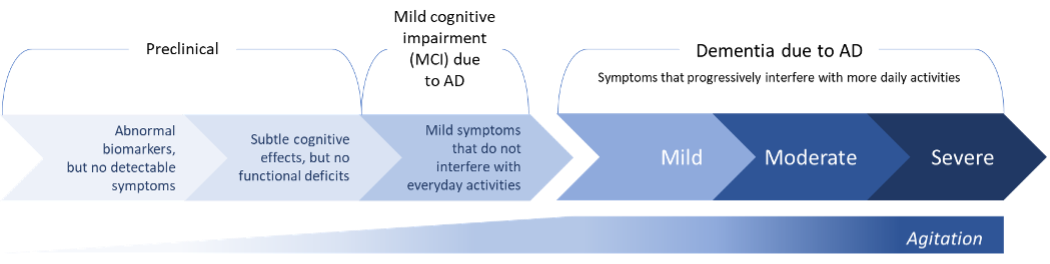
Figure 1. Alzheimer’s Disease Continuum. This figure is an illustration of the relationship between agitation and AD progression and is not intended to represent the exact prevalence or severity of agitation within the AD disease progression continuum.7
Alzheimer’s disease is characterized by a decline in cognitive function, including memory, language, and thinking skills, due to damaged neurons in the brain. As the disease progresses and neuronal damage accumulates, people may experience changes in personality, mood, or behavior.6 Most people with AD dementia will suffer from behavioral or psychological changes known as neuropsychiatric symptoms (NPS), as 98% of people living with AD dementia experience at least one NPS over the course of their disease.3 NPS is a term for a group of conditions, which can include depression, apathy, agitation, aggression, sleep disturbances, and hallucinations or delusions.3 Agitation is a common form of NPS, with an estimated 56%-75% of patients across the AD dementia severity spectrum experiencing agitation symptoms.5 Agitation can present at any time, but is more prevalent and severe in later stages of the disease.10
AAD is correlated with neurotransmitter dysregulation11,12 and abnormalities in the structure and function of brain regions associated with regulating emotions and attention.13 Noradrenaline hyperactivity, serotonergic system deficits, and dopaminergic dysfunction play roles in the dysregulation of the prefrontal cortex and the amygdala,11,12 contributing to impaired executive control and emotional drive, respectively.14,15 These evolving changes in the brain lead to prefrontal lobe and limbic system dysfunction, causing irritability and symptoms of agitation,13 especially when faced with biological, social, and environmental triggers.16,17
Behavioral and psychological symptoms are a prevalent and costly complication in the care of persons with AD, with roughly 30% of the total annual costs of caring for people with AD dementia in community dwellings spent on these symptoms.18 As one of the most complex and frequent NPS, AAD is associated with high cost and stress.3 Agitation has been associated with accelerated disease progression, more rapid functional decline, decreased quality of life for both the person living with AAD and care partners, increased risk of institutionalization, and earlier death.19-22 Additionally, behavioral disturbances like NPS are associated with higher rates of comorbidities, increased use of concomitant therapies, and greater healthcare resource utilization and cost compared to AD dementia patients without behavioral disturbances.22 AAD is also a challenge in care settings outside of the home, as agitation in long‐term care residents with dementia has been associated with greater use of medication and increased likelihood of experiencing falls, fractures, and infections compared with residents without agitation.23
In response to a lack of clarity around the description of agitation in cognitive disorders, the International Psychogeriatric Association (IPA) formed the Agitation Definition Work Group, which broadly defines agitation in cognitive disorders as occurring in patients with cognitive impairment or dementia syndrome (eg AD); exhibiting emotional distress manifesting as excessive motor activity, verbal aggression, or physical aggression; disability beyond that attributable to the cognitive impairment; and the confirmation that the agitation is not attributable solely to another psychiatric disorder or medical condition (including delirium, suboptimal care conditions, effects of a substance) (Figure 2). To meet the diagnostic criteria of agitation developed by the IPA, the person living with AD must display at least one of the three behaviors consistent with emotional distress, the state of agitation must have persisted for at least two weeks, or the behavior is a drastic change from the person’s usual behavior.24
![]()
Figure 2. IPA Definition of Agitation in Alzheimer’s Dementia (AAD)25
Identifying and Discussing AAD
Experts from the panel suggested that the disparity between the presentation of agitation symptoms and the diagnosis of AAD may partially result from gaps in understanding among the person living with AAD, care partners, and healthcare providers, due to differences in clinical and nonclinical descriptions of AAD. They agreed that these differences may impact symptom recognition and diagnosis, so there is a distinct need for materials that provide clarity around the definition of agitation with concrete, realistic examples. Given that symptom identification will most likely occur at home or in a care setting, it is critical for nonspecialists to know how agitation is defined and its implications for clinical practice. The quality and effectiveness of AAD management are dependent on clear communication and connections among the persons living with AAD, care providers, and clinicians, as the detection of NPS such as agitation is frequently based on reports from the care partner(s). A continual challenge in patient-provider dialogue is the lexicon used, as clinical and nonclinical stakeholders (such as healthcare providers and care partners) have different vocabularies for discussing AAD and its symptoms. Delays in symptom recognition due to miscommunication or inconsistent care-partner reporting can affect how early AAD is recognized, impacting clinical care for the person living with AAD.
Members of the expert panels agreed that it is of key importance for the improvement in AAD symptom recognition, diagnosis, and management that healthcare providers, particularly nonspecialists, are made aware of these lexicon challenges and encouraged to promote effective communication in patient and care-partner interactions. As a core tenet of medical engagement, cultural humility/competence may contribute to the improvement of shared understanding among people living with AAD, care partners, and healthcare professionals.25,26 The expert panelists agreed that clinical practice founded on cultural insight is a necessity for maximally effective communication with people living with AAD and care partners.
According to the expert panelists, people living with AAD and their care partners view healthcare providers as a gateway to discussion about symptoms, disease progression, and management, and believe the burden is on the clinician to initiate the conversation. Engaging in proactive discussion to encourage surveillance and description of AAD symptoms could minimize delays in diagnosis and management. Barriers to earlier care-partner reporting include social stigma, stress, and a lack of unified terminology to describe AD and AAD symptoms and their progression. Stress, burden (which increases with the severity of agitation), emotional distress, culture, educational level, and other factors may influence how care partners report symptoms.25 The expert panelists noted that care partners may make inferences about the emotional state of the individual rather than relay the specific behaviors (eg, stating the person living with AAD is anxious or frustrated instead of describing objective behaviors, such as biting or striking out); it is critical to enable care partners to clearly describe the behavior to the patient’s provider.
A strategy supported by the findings is to help the care partner(s) prepare in advance for the conversation—setting up for success can be key to increasing the rates at which people living with AAD and care partners report symptoms. This can include establishing a standard practice of using a symptom evaluation tool, such as the Neuropsychiatric Inventory Questionnaire (NP IQ), or ensuring there are ample avenues for discussion among people living with AAD, care partners and clinicians. Panelists agreed that allowing greater opportunity for the reporting of symptoms, such as a phone call or questionnaire filled out in advance of a clinical visit, can allow care partners the opportunity to bring up concerns that they may not want to discuss in front of the person living with AAD. If time permits, a separate conversation with the care partner is a valuable method to promote symptom reporting. Additionally, providing structure to the conversation using focused, guided questions may aid in identifying symptoms of AAD (See Figure 3).
![]()
Figure 3. Examples of Questions Recommended by the AAD Expert Panelists
Managing AAD: Nonpharmacologic Strategies
Nonpharmacologic management strategies are the first-line treatments for AAD.27,28 They can be simple or complex, are often used in combination, and should be customized to the individual needs of the person living with AAD.28 These strategies, encompassing mental and physical health interventions (such as cognitive behavioral therapy, therapeutic and gentle touch, or physical exercise like walks) and environmental modification (music therapy, multisensory stimulation, or creating a soothing environment) can be used to effectively help avoid or mitigate agitation episodes.28-31
Behavioral symptoms may vary throughout the day, and increased agitation, irritability, or confusion in the late afternoon and early evening, a phenomenon known as “sundowning,” may occur in people with AD dementia.31 Certain strategies, such as exposure to bright light, daily exercise, and getting enough nighttime rest, may help minimize or prevent sundowning.31 Nonpharmacologic interventions can be combined to form an individualized treatment plan for the person with AAD, as recommended by the expert panelists (Table 1). These management strategies are supported by varying quality of evidence.
Table 1: Strategies for managing agitation in Alzheimer’s dementia (AAD) 28,30,31,32-34 | |
Mental and physical health interventions | Environmental modifications |
|
|
Conclusion
Agitation in Alzheimer’s dementia is a highly prevalent condition that afflicts the rapidly growing population of aging adults.1,6 Despite significant impacts on people living with AAD and care-partner health outcomes and quality of life, AAD is underdiagnosed.1-3,5
Over the course of the panel series, the AAD experts arrived at several conclusions:
- Mutually understood communication among the healthcare provider, the person living with AAD, and care partners is essential in the diagnostic process for AAD, as miscommunication can delay diagnosis and establishment of a management plan.7
- Obstacles to improving diagnosis that were identified by panelists include inadequate interview techniques by healthcare providers and challenges in symptom identification and reporting due to cultural and language barriers.
- Differences in clinical and nonclinical lexicons may contribute to miscommunication among people living with AAD, care partners, and healthcare providers, thus negatively impacting AAD symptom identification and diagnosis.
- Cultural competency and humility are important in improving communication among healthcare providers, people living with AAD, and care partners when discussing agitation in AAD symptoms and management.
- Education directed at healthcare providers, including strategies to identify AAD symptoms, and provision of information to people living with AAD and care partners to increase symptom recognition may aid in reducing stigma and cultural and language barriers to symptom reporting.
- Clarity around the definition of agitation is needed, with concrete examples for clinicians, care partners, and people living with AAD (eg, biting, striking out); the modality and timing of the education must ensure that the information is reaching its intended audience when it is needed.
Although real-world discussion around AAD may currently lack clarity due to differences in culture and lexicon, targeted education that provides concrete AAD definitions and structure for conversations around symptoms may help to increase the identification, and promote proper management, of AAD.
Sources:
- Anatchkova M, Brooks A, Swett L, et al. Agitation in patients with dementia: a systematic review of epidemiology and association with severity and course. Int Psychogeriatr. 2019;31(9):1305-1318.
- Aigbogun MS, Cloutier M, Gauthier-Loiselle M, et al. Real-world treatment patterns and characteristics among patients with agitation and dementia in the United States: findings from a large, observational, retrospective chart review. J Alzheimers Dis. 2020;77(3):1181-1194.
- Antonsdottir IM, Smith J, Keltz M, et al. Advancements in the treatment of agitation in Alzheimer's disease. Expert Opin Pharmacother. 2015;16(11):1649-1656.
- World Health Organization. Mental health of older adults. Published October 20, 2023. Accessed May 31, 2024. https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults
- Halpern R, Seare J, Tong J, et al. Using electronic health records to estimate the prevalence of agitation in Alzheimer disease/dementia. Int J Geriatr Psychiatry. 2019 Mar;34(3):420-431.
- Alzheimer’s Association. 2024 Alzheimer’s disease facts and figures. Alzheimers Dement. 2024;20(5). Accessed May 28, 2024. https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf
- Lyketsos CG. Neuropsychiatric symptoms in dementia: overview and measurement challenges. J Prev Alzheimers Dis. 2015;2(3):155-156.
- Amjad H, Roth DL, Sheehan OC, et al. Underdiagnosis of dementia: an observational study of patterns in diagnosis and awareness in US older adults. J Gen Intern Med. 2018;33(7):1131-1138.
- U.S. Department of Health and Human Services, Food and Drug Administration. Early Alzheimer’s disease: developing drugs for treatment guidance for industry – Draft Guidance. Published March 2024. Accessed May 28, 2024. https://www.fda.gov/media/110903/download
- Lopez OL, Becker JT, Sweet RA, et al. Psychiatric symptoms vary with the severity of dementia in probable Alzheimer’s disease. J Neuropsychiatry Clin Neurosci. 2003;15(3):346-353.
- Gannon M, Wang Q. Complex noradrenergic dysfunction in Alzheimer's disease: low norepinephrine input is not always to blame. Brain Res. 2019;1702:12-16.
- Lanctôt KL, Herrmann N, Mazzotta P. Role of serotonin in the behavioral and psychological symptoms of dementia. J Neuropsychiatry Clin Neurosci. 2001;13(1):5-21.
- Rosenberg PB, Nowrangi MA, Lyketsos CG. Neuropsychiatric symptoms in Alzheimer's disease: what might be associated brain circuits? Mol Aspects Med. 2015;43-44:25-37.
- Arnsten AFT, Raskind MA, Taylor FB, et al. The effects of stress exposure on prefrontal cortex: translating basic research into successful treatments for post-traumatic stress disorder. Neurobiol Stress. 2015;1:89-99. doi:10.1016/j.ynstr.2014.10.002
- Salzman CD, Fusi S. Emotion, cognition, and mental state representation in amygdala and prefrontal cortex. Annu Rev Neurosci. 2010;33:173-202.
- Alzheimer’s Association. Anxiety and agitation. Published 2024. Accessed May 31, 2024. https://www.alz.org/help-support/caregiving/stages-behaviors/anxiety-agitation
- American Psychiatric Association. Patient and caregiver guide: antipsychotic medications to treat agitation or psychosis in adults with dementia. Accessed June 3, 2024. https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/Clinical%20Practice%20Guidelines/APA-Dementia-Patient-and-Caregiver-Guide.pdf
- Beeri MS, Werner P, Davidson M, et al. The cost of behavioral and psychological symptoms of dementia (BPSD) in community dwelling Alzheimer's disease patients. Int J Geriatr Psychiatry. 2002;17(5):403-408.
- Peters ME, Schwartz S, Han D, et al. Neuropsychiatric symptoms as predictors of progression to severe Alzheimer's dementia and death: the Cache County Dementia Progression Study. Am J Psychiatry. 2015;172(5):460-465.
- Scarmeas N, Brandt J, Blacker D, et al. Disruptive behavior as a predictor in Alzheimer disease. Arch Neurol. 2007;64(12):1755-1761.
- Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of behavioral and psychological symptoms of dementia. BMJ. 2015;350:h369.
- Aigbogun MS, Stellhorn R, Hartry A, et al. Treatment patterns and burden of behavioral disturbances in patients with dementia in the United States: a claims database analysis. BMC Neurol. 2019;19(1):33.
- Fillit H, Aigbogun MS, Gagnon-Sanschagrin P, et al. Impact of agitation in long-term care residents with dementia in the United States. Int J Geriatr Psychiatry. 2021;36(12):1959-1969.
- Sano M, Cummings J, Auer S, et al. Agitation in cognitive disorders: progress in the International Psychogeriatric Association consensus clinical and research definition. Int Psychogeriatr. 2024;36(4):238-250.
- Stella F, Forlenza OV, Laks J, et al. Caregiver report versus clinician impression: disagreements in rating neuropsychiatric symptoms in Alzheimer's disease patients. Int J Geriatr Psychiatry. 2015;30(12):1230-1237.
- Lekas HM, Pahl K, Lewis CF. Rethinking cultural competence: shifting to cultural humility. Health Serv Insights. 2020;13:1178632920970580.
- O'Gorman C, Khoury R, Anderson A, et al. A framework for developing pharmacotherapy for agitation in Alzheimer’s disease: recommendations of the ISCTM* working group. J Prev Alzheimers Dis. 2020;7(4):274-282.
- Ijaopo EO. Dementia-related agitation: a review of non-pharmacological interventions and analysis of risks and benefits of pharmacotherapy. Transl Psychiatry. 2017;7(10):e1250.
- Lyketsos CG, Colenda CC, Beck C, et al. Position statement of the American Association for Geriatric Psychiatry regarding principles of care for patients with dementia resulting from Alzheimer disease. Am J Geriatr Psychiatry. 2006;14(7):561-572.
- National Institute on Aging. Coping with agitation and aggression in Alzheimer's disease. Updated May 17, 2017. Accessed June 3, 2024. https://www.nia.nih.gov/health/coping-agitation-and-aggression-alzheimers-disease
- National Institute on Aging. Tips for coping with sundowning. Updated May 17, 2017. Accessed June 3, 2024. https://www.nia.nih.gov/health/tips-coping-sundowning
- Martín-García A, Corregidor-Sánchez AI, Fernández-Moreno V, et al. Effect of doll therapy in behavioral and psychological symptoms of dementia: a systematic review. Healthcare (Basel). 2022;10(3):421.
- Telhede EH, Arvidsson S, Karlsson S. Nursing staff's experiences of how weighted blankets influence resident's in nursing homes expressions of health. Int J Qual Stud Health Well-being. 2022;17(1):2009203.
- Thunberg S, Rönnqvist L, Ziemke T. Do robot pets decrease agitation in dementia patients? An ethnographic approach. Social Robotics. 2020:616-627.
Author information:
Lead author
Jeff Cummings, MD, ScD
University of Nevada, Las Vegas
Corresponding author
Carolyn Clevenger, DNP, RN, GNP-BC, FAANP, FGSA, FAAN
Email: carolyn.clevenger@emory.edu
Telephone: 404-712-2394
Contributing authors
Tatyana Gurvich, PharmD, BCGP
USC School of Pharmacy
Lakelyn Hogan Eichenberger, PhD, MA, MBA
Home Instead
W. Clay Jackson, MD, DipTh
University of Tennessee College of Medicine
Sean Tunis, MD, MSc
Rubix Health
Kate Zhong, MD, MSc, FRCP
University of Nevada, Las Vegas