
Who Cares for the Caregiver?
Case Presentation
Mrs. S is a 55-year-old married woman who is employed in the Finance department of a community college. She has two children. Her older son recently graduated from college and moved across the country to attend graduate school; her younger son, age 20, has Down’s syndrome, lives at home, and attends a daily workshop program where he is learning life skills with the goal of eventually moving to his own apartment. Mrs. S has been married for 35 years. Her husband had been recently diagnosed with prostate cancer and underwent surgery followed by radiation therapy for a high-grade malignancy. His illness and her son’s move were stressful events for Mrs. S, but she had begun to feel that everything was returning to a more manageable state. During her husband’s illness, she fell behind in her own medical appointments and knows that she is overdue for a mammogram and general check-up. Mrs. S has had hypertension for many years, but her blood pressure has been controlled on lisinopril 20 mg with hydrochlorothiazide 25 mg once daily.
Mrs. S receives a telephone call one day while at work from the local police in the town where her 87-year-old mother has been living in the family home. Her mother, Mrs. D, was found wandering on the highway in a confused and disheveled state. She was taken to a local hospital where she was admitted due to dehydration and concerns regarding her malnourished state. Mrs. S makes arrangements for a neighbor to check in on her husband and son, and is able to take a few days off from work. She travels to see her mother and is shocked to find her confused, thin, and frail. Mrs. S realizes that she has relied on weekly telephone calls with her mother instead of visits since her husband became ill. When she visits her mother’s house, she finds it in disarray, with little food, unwashed dishes, and piles of unopened mail. Mrs. D responds well to hydration and nutritional support in the hospital. No cause can be found for her confusion, and she is diagnosed with Alzheimer’s dementia. Mrs. S realizes that her mother cannot be left alone and decides to bring her to her apartment to live with her and her husband and disabled son.
Mrs. S soon finds that she is devoting increasing hours each day to the needs of her family. She gets up before 5:00 AM each day to prepare meals for her husband and mother. She helps her son get ready to catch the bus to his day center, and then goes to work at her full-time job. Even with the assistance of neighbors who check on her husband and mother, she has had to leave work early several times when called about her mother wandering outside of the building. When she returns home from work in the evenings, Mrs. S typically finds her apartment full of dirty dishes and soiled laundry, and her husband and mother arguing with each other. Her son’s performance in his job program has declined because Mrs. S has been unable to help him practice his assignments at home. Mrs. S feels determined to keep her family together but starts feeling tired all of the time.
One day at work, Mrs. S develops a throbbing headache, one in the latest of a series of aches and pains. She takes a break and develops blurred vision while walking to the bathroom. One of her coworkers notes how unsteady she appears and calls an ambulance. Mrs. S is taken to the Emergency Room, where she is found to have a blood pressure of 220/160 mm Hg. She also is found to have a cardiac arrhythmia, and the physician wants to admit her to the hospital Telemetry unit for monitoring and treatment of her hypertension. Mrs. S bursts into tears, insisting that she cannot be admitted to the hospital. She reports that she has to go home to care for her family and wants to leave the hospital. The Emergency Room staff feels that she is depressed and requests both social service and psychiatry consultation.
Discussion
Women are frequently the major caregivers in both formal and informal roles.1 While caregiving is associated with many positive aspects, the stresses and burdens of the caregiver role pose many challenges for women’s health.2,3 The case of Mrs. S illustrates how a working mother gradually takes on the role of caregiver to a disabled son, a husband with cancer, and a mother with dementia. As populations continue to age, many caregivers find themselves dealing with elderly parents, spouses, and children with needs.4 Caregiving is becoming more common and more complex.5 Family caregivers are often referred to as “informal,” as their work is unpaid and often unrecognized.1 While family caregivers come from many diverse backgrounds, the most common features include women in their 50s and 60s who are married, employed outside of the home, and provide care to elderly relatives and often their spouses and children or grandchildren.6 While there has been some increase in the number of male caregivers, women still provide the majority of family caregiving and carry the greatest burden of multiple caregiver roles. It is estimated that 30% of the population provides caregiving services to relatives, and 80% of these caregivers are women.6,7
Caregivers provide assistance with services that range from bill paying to shopping to personal care needs such as bathing and grooming. While paid, or “formal,” caregivers typically have training and a clear job description, family caregivers frequently provide all of the care necessary to keep their relative at home and safe in the community.8,9 It is the open-ended nature of this role that often leaves caregivers feeling frustrated and overwhelmed.5,6 Many caregivers become isolated from friends and other family members. Most caregivers neglect their own personal health needs and medical appointments in order to accommodate their increasing responsibilities. This leaves them vulnerable to illness, stress, and depression.4-7
It is vital that clinicians screen caregivers for signs of depression, anxiety, and burden. A useful tool that assesses the psychological, social, financial, and physical burdens of caregiving is the Caregiver Strain Index.10,11 This 13-item scale is easily administered and can guide the clinician in the areas causing distress to the caregiver.11 Caregivers who are stressed are more likely to have depression, anxiety, and cardiovascular disease.12 Caregiver stress has been associated with premature nursing home placement of patients with dementia.8
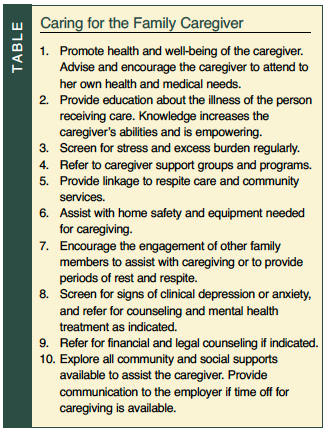
Interventions to assist caregivers with their tasks have been developed1,5-7,9 (Table). Educational programs designed to promote coping skills and increase knowledge have been shown to reduce symptoms of burden and depression.5,7 Interventions that address multiple components, including social support, caregiving skills, reducing stress, and depression, have shown a positive impact on both caregivers and patients.1,4 Day care and respite care programs are often valuable for the caregiver who is facing an immediate need for assistance.4 Treatment of the caregiver who has depression, anxiety, sleep disturbances, or other psychiatric symptoms is vital and may include medications, psychotherapy, or a combination of both.5-7 Caregiver support groups enable members to expand their social networks, reduce isolation, and increase mastery of caregiving techniques.1,4
Information for caregivers can be accessed and downloaded from the National Alliance for Caregiving website at www.caregiving.org, the Alzheimer’s Association at www.alz.org, and the Alzheimer’s Foundation of America website at www.alzfdn.org.
Outcome of the Case Patient
 Mrs. S was evaluated in the Emergency Room by the psychiatrist and the social worker. She appeared tired and anxious, and was tearful throughout most of the interview. Mrs. S reported that she felt overwhelmed and unable to keep up with all of the needs of her family and her job. She worried constantly about the health of her husband, mother, and son, as well as trying to manage the family finances with her husband unable to work. She described often crying at her desk at work, feeling guilty that she could not keep up with her family’s needs, and frustrated by the amount of work she faced each night when she arrived home. Mrs. S missed several doctors’ appointments because she had no one to stay with her mother. She described how isolated she had become, feeling alone and often frightened. Mrs. S admitted that she wanted to get help for herself but always placed her family first. The psychiatrist explained that Mrs. S needed to care for herself in order to help her family; it was time to care for the caregiver. She agreed to stay in the hospital for treatment if someone would call a neighbor to stay with her family.
Mrs. S was evaluated in the Emergency Room by the psychiatrist and the social worker. She appeared tired and anxious, and was tearful throughout most of the interview. Mrs. S reported that she felt overwhelmed and unable to keep up with all of the needs of her family and her job. She worried constantly about the health of her husband, mother, and son, as well as trying to manage the family finances with her husband unable to work. She described often crying at her desk at work, feeling guilty that she could not keep up with her family’s needs, and frustrated by the amount of work she faced each night when she arrived home. Mrs. S missed several doctors’ appointments because she had no one to stay with her mother. She described how isolated she had become, feeling alone and often frightened. Mrs. S admitted that she wanted to get help for herself but always placed her family first. The psychiatrist explained that Mrs. S needed to care for herself in order to help her family; it was time to care for the caregiver. She agreed to stay in the hospital for treatment if someone would call a neighbor to stay with her family.
The hospital social worker explained that Mrs. S and her family were eligible for a respite care program that provided visiting social work and nursing services with home health aides to assist with care while she was in the hospital. In addition, she told Mrs. S about a number of day care programs for patients with Alzheimer’s dementia that her mother might benefit from. There were also services available for her husband through the hospital’s cancer outreach program. Mrs. S felt reassured and allowed herself to undergo the medical care she clearly needed.
While in the hospital, the psychiatrist continued to see Mrs. S, who underwent cardiac catheterization and adjustment of her blood pressure regime. She continued to appear depressed and anxious, with periods of tearfulness and almost constant worry. Mrs. S was started on citalopram 20 mg once daily for depression, and upon discharge on the seventh hospital day was referred to the hospital’s caregiver support group.
At a 6-month follow-up visit with the psychiatrist, Mrs. S was no longer feeling depressed and was coping better with her complex role. While she was still the main caregiver for her family, she enrolled her mother in a day care program that provided transportation and meals. Her husband was able to return to work part time and also assisted more with the household chores. Mrs. S began attending a caregiver support group and realized that she needed to make time for herself. She consulted with an eldercare attorney to assist with her mother’s finances, house, and estate planning. Mrs. S reported that her older son returned home more often from graduate school to provide assistance with the family, and that she felt more comfortable asking for help. Mrs. S continues on the citalopram 20 mg daily and sees both her psychiatrist and primary care physician on a regular basis.
The author reports no relevant financial relationships.
Dr. Lantz is Chief of Geriatric Psychiatry, Beth Israel Medical Center, First Ave @ 16th Street #6K40, New York, NY 10003; (212) 420-2457; fax: (212) 844-7659; e-mail: mlantz@chpnet.org.