
Peer Reviewed
What is this asymptomatic inflamed streak?
Dermclinic
A Photo Quiz to Hone Dermatologic Skills

Case 1:
A 5-year-old girl is brought for evaluation of an asymptomatic inflamed streak on one leg that has been present for several weeks. She is otherwise healthy and takes no medications.
What does this look like to you?
A. Psoriasis.
B. Contact dermatitis.
C. Lichen planus.
D. Lichen striatus.
E. Lichen sclerosus.
Answer on next page.
Case 1: The child has lichen striatus, D, a self-limited papular eruption that occurs primarily in children and affects twice as many girls as boys. The eruption persists for months before resolving spontaneously. No treatment is necessary, although some lesions respond to topical corticosteroids.
Psoriasis consists of discrete scaly lesions. Contact dermatitis is pruritic. Lichen planus features discrete flat-topped polygonal purple papules. Lichen sclerosus is characterized by hypopigmented coalescing macules.
Case 2 on next page

Case 2:
A 7-year-old boy has had an asymptomatic papular eruption on the trunk and extremitiesfor several weeks. He is otherwise healthy.
What is your clinical impression?
A. Follicular eczema.
B. Pityrosporum folliculitis.
C. Lichen nitidus.
D. Lichen planus.
E. Keratosis pilaris.
Answer on next page.
Case 2: Lichen nitidus, C, a condition of unknown cause sometimes seen in children, generally lasts for several months before resolving. There is no known treatment.
Follicular eczema is usually seen only in atopic persons. Pityrosporum folliculitis is typically confined to the trunk. Lichen planus is pruritic and consists of flat purple polygonal papules. Keratosis pilaris preferentially affects atopic persons and is confined to the upper outer arms, upper outer thighs, and cheeks.
Case 3 on next page
 Case 3:
Case 3:
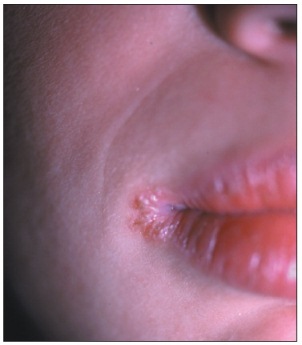
Irritation at the angle of the lips on the right side bothers a 14-year-old boy. The rash failed to respond to an antifungal cream prescribed by another practitioner. The patient has been using isotretinoin( for acne for 3 months.
Which of the following do you suspect?
A. Resistant candidal infection.
B. Contact dermatitis from lip balm.
C. Contact dermatitis from toothpaste.
D. Staphylococcal infection.
E. Irritation caused by a vitamin deficiency.
Your next step is to . . .
F. Recommend more frequent use of lip balm.
G. Recommend achange in the brand of oral hygiene products used.
H. Prescribea different topical antifungal.
I. Order a bacterial culture.
J. Prescribe vitamin B12 supplements or injections.
Answers on next page.
Case 3: A culture of material from this patient's lip, I, confirmed an angular cheilitis caused by Staphylococcus aureus, D. A Candida infection can mimic this bacterial condition; if the patient's disease fails to respond to antifungal therapy, mupirocin( cream may be tried or a bacterial culture can be performed.
Contact dermatitis to oral hygiene products usually produces a circumferential swelling around the vermilion border of the lips. The eruption caused by a vitamin B12 deficiency typically is bilateral.
Most likely, isotretinoin-induced dryness of the lips predisposed this patient to cheilitis, as well as to the staphylococcal infection. The patient was advised to use lip moisturizer, F, regularly. Mupirocin cream quickly cleared the infection. The patient has had no further episodes.