
The Weekend Athlete: Common Foot and Ankle Injuries
ABSTRACT: Physical activity is becoming an increasingly popular lifestyle choice as people are encouraged to make healthier choices. Extreme sports, such as running marathons, have become mainstream, resulting in a higher incidence of training injuries that stem from individuals with previously low levels of activity prepping for high-intensity workouts. Primary health care providers must diagnose and manage many common lower extremity injuries and refer severe injuries to specialists. This article will focus on the evaluation, diagnosis, and management of 4 common foot and ankle injuries.
Ankle sprains are one of the most common sports injuries that primary care or emergency room physicians see for evaluation and treatment. Almost 1 million people are evaluated each year for an ankle sprain and account for 25% of all sports-related injuries.1 Overall, incidence of ankle sprain is 2.15 per 1,000 person-years and is highest in the 15 to 19 age group at 7.2 per 1,000 person years.2
ANKLE SPRAINS
There are 3 types of ankle sprains: lateral, medial, and syndesmotic injuries (referred to as high ankle sprains). The most common mechanism of injury to the ankle is plantar inversion while the foot is plantar flexed. This causes a lateral sprain, which represents 85% of all ankle sprain injuries,3 and is most common due to the anatomy of the ankle—lateral structures are weaker than the medial.
It is less common to evert the ankle and cause damage to the much stronger medial deltoid ligament complex; dorsiflexion and eversion can also cause an injury to the syndesmotic structures—the tibiofibular ligament. Although the principles of diagnosis, treatment, and rehabilitation apply to all types, we will focus on the lateral ankle sprain.
The lateral ligament complex is made of 3 ligaments: anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL) (Figure 1).4 Grading of ankle sprains is calculated using the AMA guidelines: grade I equals mild or no tearing; grade II means moderate or partial tearing, and grade III corresponds to severe or complete rupture of the ligament.5 Grading is often very difficult secondary to pain and swelling. In addition, studies have shown that grading is not all that accurate.6 However, it is of clinical use to identify severe instability on exam as this may denote prolonged healing times.

Figure 1. Lateral ankle sprain is the most common ankle injury with the mechanism of injury being plantar inversion.
Diagnosis
Proper diagnosis requires obtaining a thorough history including mechanism of injury, ability to walk after injury, location of pain, and previous injury to the ankle. Start by examining the uninjured ankle to reduce the patient’s anxiety, as well as have a basis for comparison and a reference to anatomy and stability.
Common ankle sprains may have significant edema but if they have gross deformities, a fracture should be suspected. The presence of localized edema or ecchymosis may further guide your exam. Direct pressure of the ATFL, CFL, PTFL, medial deltoid ligament complex, the full length of the tibia and fibula, and Achilles tendon is needed to assess for pain, edema, and crepitus. This helps grade the severity of the injury and guide treatment, prognosis, and recovery time to normal athletic activity. To test, have the patient actively move the joint through all planes of motion. The clinician should then passively move the affected ankle in plantar flexion, dorsiflexion, inversion, and eversion as well as combination of inversion/eversion with flexion.
Specific tests can further evaluate the extent of the injury. Most ankle injuries result in a lateral ankle sprain, but a small proportion can result in injuries accompanied by significant morbidity if not diagnosed and treated properly.
• Anterior drawer test. This is used to assess the anterior talofibular ligament, but is more reliable if performed within 48 hours of the injury. The clinician places one hand above the joint line and cups the heel with the other hand with force pulling the heel anterior. A shift of greater than 3 mm indicates a positive anterior drawer sign.3
• Talar tilt test. To examine the deltoid and lateral ligaments using eversion and inversion stresses.3
• Thompson test. An Achilles tendon rupture may be missed if a Thompsontest is not performed. The Thompson test is performed by gripping the mid-calf with the knee at 90° and observing for plantar flexion on the foot to show the Achilles tendon is still intact. Lack of plantar flexion would suggest Achilles tendon rupture.3
• Squeeze test. This test is a crucial part of any ankle exam as it evaluates for syndesmosis injury or high ankle sprain. It is performed by squeezing the mid-calf portion of the lower extremity to push the tibia and fibula together and is positive if pain is elicited distally in the region of the tibia-fibular syndesmosis. The external rotation test for syndesmotic injury is performed by placing a supporting hand on the lower extremity above the joint line and providing external rotation to elicit pain in the syndesmotic region. The clinician should also examine and document neurological and vascular competency in the injured leg.
• Pain-free direct pressure. The fifth metatarsal can be injured in 2 important ways that can be ruled out by pain-free direct pressure. Those injuries are an avulsion fracture of the peroneal brevis tendon at the base of the fifth metatarsal or a fracture of the proximal fifth metatarsal, commonly called Jones fracture.
A Maisonneuve fracture involves the proximal fibula in conjunction with a syndesmosis injury, which would be found with palpation of the entire fibula. An osteochrondral talar dome lesion may be suggested if pain or edema is noted along the talocrurual joint line. Peroneal strains or dislocation are evaluated by eversion of the ankle against resistance.
Treatment
The treatment approach consists of reducing swelling and inducing early mobilization to reduce the amount of mobility and strength that could be lost. The initial treatment includes the combination of protection, rest, ice, compression, and evaluation (PRICE). Commercially-available plastic or lace-up fabric braces can provide protection from further injury. If the patient is initially unable to bear weight on the injured ankle, crutches should be used until weight bearing ability is restored.
Cryotherapy is applied on medial and lateral areas of the ankles for 20 minutes every 2 to 3 hours for the first 3 to 7 days.9-11 Compression can be obtained by an ace bandage in conjunction with a felt U-shaped device, which covers lateral and medical surfaces, or a donut device made specifically to encircle the lateral and medial malleolus. Commercially-available devices, such as air stirrups, can also provide support and compression. During this time, the injured extremity is elevated to reduce edema. Prolonged casting is detrimental compared with early mobilization.4,12
Once edema is reduced, the treatment plan should consist of the following exercises: range of motion, strength training, proprioception, and training for specific activities. Range of motion can be addressed early with instructions to draw the letters of the alphabet with the injured big toe throughout the day, along with Achilles tendon stretches by using a towel looped over the injured plantar surface to be pulled toward the body using the arms. When full range of motion is evident by the ability to walk pain free, strength training may begin.
Strength training may consist of isometric, manual resistance, or elastic tubing exercises. These workouts are to be continued until the number of repetitions and resistance are symmetrical between the injured and uninjured limb. Proprioception can be relearned with a wobble board or by brushing one’s teeth while balanced on the injured foot. Lastly, activity-specific exercises—ie, walking and running, figure 8 drills, jogging, sprinting, circles, cutting, pivoting, and jumping—are reintroduced. Prior studies have shown the aforementioned conservative approach to provide a faster turnaround to normal athletic activity than surgical intervention.13,14
The recovery time to return to sports depends on the grade of the injury and the time and effort put into rehabilitation. On average, a grade I sprain will result in athletic inactivity for 11 days; grade II for 2 to 6 weeks; and a grade III for 4 to 26 weeks.1 The largest risk factor for an ankle sprain is a previous ankle sprain. A review by Thacker et al shows that athletes with a sprained ankle should achieve complete rehabilitation before returning to sport activity and athletes with moderate or severe ankle sprain should wear an appropriate orthosis for at least 6 months.14 New research finds that ankle bracing may decrease rate of recurrence in high risk recreational activities.15
PLANTAR FASCIITIS
Plantar fasciitis is the most common causes of plantar heel pain in America. It accounts for about 600,000 office visits a year and affects about 10% of the population.16 Predisposing factors include obesity, flat feet (pes planus) or high arches (pes cavus), prolonged standing, or certain activities including dancing and running. In young athletes, this pain often follows a sudden increase in training intensity or running distance. It is proposed that walking barefoot on concrete or other hard surfaces may predispose to this condition (although this condition can occur in people of any age without any predisposing factors).16 The cumulative trauma to the thick aponeurosis, which gives support to the arch of the metatarsal area, generates the pain. This condition is clinically diagnosed—with about 80% of patients seeing self-limiting resolution within 1 year, although no strong evidence suggests any particular treatment is beneficial.16

Diagnosis
The hallmark symptom for diagnosis is inferior heel pain that is worse with the first step of the day, improves with warm-up and then worsens again with prolonged movement.
Physical exam should show point tenderness to the medial calcaneal tubercle or insertion of the plantar fascia. Physical exam may also reveal point tenderness along the plantar aponeurosis with dorsiflexion of the toes/foot.
Radiologic studies cannot make a diagnosis, but do help rule out other conditions. The presence of a heel spur on x-ray does not aid in diagnosis since 50% of patients with plantar fasciitis reveal a heel spur and 19% of patients without plantar fasciitis also have heel spurs.16 A bone scan can show increase uptake at the medial calcaneal tuberosity, and an ultrasound and MRI can reveal thickened plantar fascia, but in general, radiology is not helpful unless conservative measures fail.
The most common differential diagnoses include plantar fascia rupture, tarsal tunnel, heel pad atrophy, and painful heel pad.
Treatment
No single method of treatment has shown strong evidence of effectiveness. Since most conservative therapies are easy, safe, and inexpensive, they are worth an initial trial. Reasonable treatments include ice, rest, and a dose of nonsteroidal anti-inflammatory medications (NSAIDs), which are the hallmark of musculoskeletal medicine and may give some initial relief.
Custom-made and prefabricated shoe inserts should be considered in early conservative treatment, especially for patients with pes planus. One study showed prefabricated shoe inserts being superior over custom inserts.16,17 Another study showed 72% of patients improved with stretching alone, 90% improved with stretching in conjunction with a silicone or rubber heel cup, while adding a custom-made orthotic showed no benefit over stretching alone.18
A simple initial treatment plan consists of 8 weeks of stretching the Achilles and plantar fascia combined with a prefabricated heel insert or orthotic. Plantar fascia stretching seems to be the most beneficial using exercises such as toe curls, toe towel curls, and simple forced dorsiflexion of the foot and toes. Night splints, which maintain ankle and toe dorsiflexion, allow mild stretching consistently throughout the night. There is no strong evidence that supports prefabricated versus custom night splints.16,18 If these conservative measures fail, a corticosteroid injection could be considered although pain relief has only been demonstrated at 1 month with no significant difference at 6 months.16
Extracorporeal shock wave ultrasound therapy had previously been shown to benefit runners only, but now studies have shown mixed results with some possibly positive benefit.16,18 Casting has also shown minimal to no benefit in treatment.16
Lastly, surgical therapy can be entertained if conservative measures fail to treat the ongoing symptoms. No randomized, controlled studies have assessed the effectiveness of surgical intervention, but retrospective studies show relief in 75% to 95% of patients.16 Patients are able to return to sports when no longer symptomatic.
 ACHILLES TENDON
ACHILLES TENDON
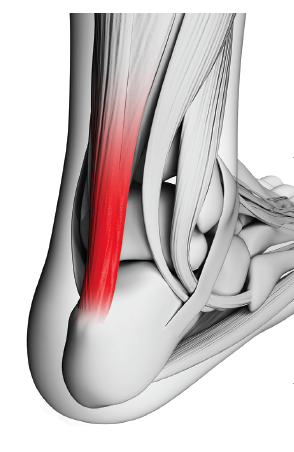
The Achilles tendon is a very large tendon that is vulnerable to injury due to limited blood supply and the magnitude of forces applied during recreational sports. The arteries run longitudinally along the muscle and provide minimal blood supply at 2 cm to 6 cm from the insertion into the calcaneus. During normal walking, the tendon stretches and glides with the degree of foot motion, which puts repetitive and cumulative forces on the complex. These forces are magnified up to 8 times the body weight with running and jumping. For these reasons, the Achilles tendon is vulnerable to tendonitis, peritendinitis, tendonosis, bursitis, and rupture.
Diagnosis
A careful history and physical exam includes details regarding training intensity, duration, ground surfaces, and other pertinent information. This condition often coincides with a sudden increase in training. Physical examination should include an inspection of shoes, observation of gait, biomechanics, and shoe age.
The presenting symptom is most often pain or tenderness proximal to the insertion at the calcaneus and is often insidious in onset and accompanied by stiffness. This pain initially improves with warm-up exercises but is worsened with further activity. Physical exam will show point tenderness at the insertion or just proximal to the calcaneus.
In contrast, peritendinitis will cause pain along the entire Achilles tendon with gentle rubbing between fingers. Foot dorsiflexion often exacerbates the pain. A thick and tender bursa at the insertion of the Achilles at the calcaneus would signify bursitis. Physical exam should differentiate these injuries from Achilles rupture, which can be easily missed in up to 25% of injuries.19
The Thompson’s test involves squeezing of the calf muscle and produces foot dorsiflexion if the tendon is at least partially intact. Other historical clues such as sudden onset and a loud popping sound would likely indicate an Achilles tendon rupture. These soft tissue injuries do not often require plain radiographs, but may require an occasional MRI for confirmation of injury and/or surgical planning for complete rupture.
Treatment
Achilles tendonitis, peritedonitis, tendonosis, and bursitis are all treated similarly with the exception that corticosteroid injections are more appropriate for treating bursitis.19 This common treatment includes rest, ice massage, NSAIDs, and stretching. The stretching portion involves posterior leg stretching using a wall or doorway, calf plantar fascia stretching, and toe raises. Evidence from clinical studies and best outcomes for Achilles tendonopathy have been achieved with eccentric calf exercises.20
A change in footwear, heel inserts, or orthotics may also be helpful. Proper education of athletes for warm-up and stretching before and after athletic activity helps prevent re-injury. It is important to identify an Achilles rupture, since treatment involves immobilization or surgery. All of these conditions have an excellent prognosis and return to sports following appropriate treatment and therapy.
METATARSAL STRESS FRACTURES
Stress fractures occur as a result of repetitive injury that overwhelms the ability of the bone to repair itself. Any recreational or sports activity that requires running or jumping can predispose to stress fractures. Among athletes with stress fractures, the metatarsals are involved 25% of the time.21
Stress fractures are most commonly due to a sudden increase in activity beyond current athletic capacity, leading to bony microtrauma. Metatarsal stress fractures occur most commonly in the distal second and third metatarsals and less commonly in the fifth. The fifth metatarsal stress fracture must be differentiated from Jones fracture, which is more serious and difficult to heal.
Diagnosis
Patient history often reveals an insidious onset of pain in the midfoot area, which worsens with activity or weight bearing in a patient with a recently increased level of exercise intensity. The clinician should ask specifically about changes in shoe wear, running surfaces, increases in training, increases in intensity, and frequency. The physical exam will show point tenderness along the offending metatarsal, sometimes accompanied with edema and ecchymosis. Initial radiographs may not show any acute changes. Follow-up radiographs show periosteal thickening in 50% of cases.21
Narrowing of the medullary canal, cortical hypertrophy, faint lucency, and periosteal thickening develop first. This is followed by a callus formation, sometimes as early as 4 to 5 weeks after the onset of symptoms. Distinct, well-organized callus is usually seen after several months. MRI and 3-phase nuclear medicine scans can reveal pathology earlier than plain radiograph.
Treatment
Initial treatment may depend on the site of stress fracture and severity of pain. Fifth metatarsal stress fractures classically have a high rate of nonunion, but are fortunately rare occurrences.22 However, if a fifth metatarsal lesion is suspected or diagnosed, referral to orthopedist is warranted for surgery. Any fracture with evidence of displacement should be referred for further evaluation by an orthopedist.
Otherwise, let the patient’s pain guide your treatment. For severe pain with normal activities, management should include walking using crutches and avoiding weight bearing on the injured structure. Less severe pain may require using crutches for limited weight bearing, in conjunction with a short leg cast or a prefabricated walker boot. These patients should be transitioned to progressive weight bearing with a hard-soled shoe, followed by a well-padded shoe—using pain levels to guide further management.
Avoiding activities that aggravate the injury is recommended for 4 to 8 weeks in conjunction with ice therapy. Athletes are advised to continue athletic training with cross-training in low impact sports. NSAIDs are controversial as some propose that they can affect bone healing.
Remember to identify any correctable factors that contributed to the stress fracture such as training surface, biomechanics, or training equipment. Injury prognosis is good, although the treatment course is often lengthy. Patients are advised to gradually return to sports with ample stretching and warm up to decrease recurrence of injury.
The primary care provider will continue to be presented with patients who are new to sports, long time athletes, or engaging in what was previously rare events like marathons and thus with common foot and ankle injuries. This article should help with evidenced-based proper diagnosis, treatment, and need to refer for further consultation. ■
Ottawa Ankle Rules
The Ottawa ankle rules were developed to reduce the amount of radiographs used in evaluating ankle injuries since the vast majority is interpreted as normal. These guidelines have been shown to provide near 100% sensitivity and have a pooled negative likelihood ratio of 0.08.7,8 Similarly, near 100% sensitivity and pooled negative likelihood ratio of 0.07 have been found in children older than the age of 5.8
According to the Ottawa ankle rules, radiography is required to rule out a fracture if there is bone tenderness to the inferior 6 cm posterior portion or tip of the medial and lateral malleolus, proximal fifth metatarsal, and navicular; or the inability to bear weight of 4 steps at time of injury or in the clinician’s office. Radiographic evaluation consists of anterior-posterior, lateral, and mortise views of the ankle and foot to access for evidence of fracture or syndesmosis injury. Further radiographic evaluation such as computed tomography or magnetic resonance imaging (MRI) is not necessary in the acute setting, but can be useful if chronic pain or instability become an issue.
References:
1.Hockenburry RT, Sammarco GJ. Evaluation and treatment of ankle sprains: clinical recommendations for a positive outcome. Phys Sportsmed. 2001;29(2):57-64.
2.Waterman BR, Owens BD, Davey S, et al. The epidemiology of ankle sprains in the United States. J Bone Joint Surg Am. 2010;92(13):2279-2284.
3.Trojian TH, McKeag DB. Ankle sprains: expedient assessment and management. Phys Sportsmed. 1998;26(10):29-40.
4.Kannus P. Immoblization or early mobilization after an acute soft tissue injury? Phys Sportsmed. 2000;28(3):55-63.
5.Taylor DC, Arcerio RA, Kirkendall DT, Garrett WE Jr. Sports medicine terminology. In: DeLee J, Drez D, Miller M, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia, PA: Saunders Elsevier; 2009:2207.
6.Frey C, Bell J, Teresi L, et al. A comparison of MRI and clinical examination of acute lateral ankle sprains. Foot Ankle Int. 1996;17(9):533-537.
7.Jenkin M, Sitler MR, Kelly JD. Clinical usefulness of the Ottawa Ankle Rules for detecting fractures of the ankle and midfoot. J Athl Train. 2010;45(5):480-482.
8.Bachmann LM, Kolb E, Koller MT, et al. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ. 2003;326(7386):417.
9.Hubbard TJ, Denegar CR. Does cryotherapy improve outcomes with soft tissue injury? J Athl Train. 2004;39(3):278-279.
10.Hubbard TJ, Aronson SL, Denegar CR. Does cryotherapy hasten return to participation? A systematic review. J Athl Train. 2004;39(1):88-94.
11.Bleakley C, McDonough S, MacAuley D. The use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sports Med. 2004;32(1):251-261.
12.Kerkhoffs GM, Rowe BH, Assendelft WJ, et al. Immobilisation and functional treatment for acute lateral ankle ligament injuries in adults. Cochrane Database Syst Rev. 2002;(3):CD003762.
13.Wolfe MW, Uhl TL, Mattacola CG, McCluskcey LC. Management of ankle sprains. Am Fam Physician. 2001;63(1):93-104.
14.Thacker SB, Stroup DF, Branche CM, et al. The prevention of ankle sprains in sports. A systemic revue of the literature. Am J Sports Med. 1999;27(6):753-760.
15.Handoll HH, Rowe BH, Quinn KM, de Bie R. Interventions for preventing ankle ligament injuries. Cochrane Database Syst Rev. 2001;(3):CD000018.
16. Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. Am Fam Physician. 2005;72(11):2237-2242.
17.Orchard J. Plantar fasiitis. BMJ. 2012;345:e6603.
18.Crawford F, Thomson C. Interventions for treating plantar heel pain. Cochrane Database Syst Rev. 2003;(3):CD000416.
19.Mazzone MF, McCue T. Common conditions of the achilles tendon. Am Fam Physician. 2002;65(9):1805-1810.
20.Asplund CA, Best TM. Achilles tendon disorders. BMJ. 2013;346:f1262.
21.Sanderlin BW, Raspa RF. Common stress fractures. Am Fam Physician. 2003;68(8):1527-1532.
22.Bruckner P, Bradshaw C, Bennell K. Managing common stress fractures: let risk level guide treatment. Phys Sportsmed. 1998;26(8):39-47.
Ryan Fowler, MD, lives in Temple, TX where he is a family physician with a focus on primary care sports medicine. He stays active with functional fitness, hiking, cycling, and chasing after his three boys.