
Peer Reviewed
A Truck Driver With a Skin Lesion on His Upper Arm
AUTHORS:
Nguyet-Cam V. Lam, MD, and Neil B. Matalia, MD
CITATION:
Lam NCV, Matalia NB. A truck driver with a skin lesion on his upper arm. Consultant. 2016;56(12):1093.
An 85-year-old white male truck driver presented with a skin lesion on his left upper arm, approximately 5 cm above the elbow. He had noticed the lesion approximately 2 months ago as it slowly enlarged and became tender. The lesion often got caught in his sleeve and subsequently bled. He is a former smoker, and he has a history of renal cell carcinoma.
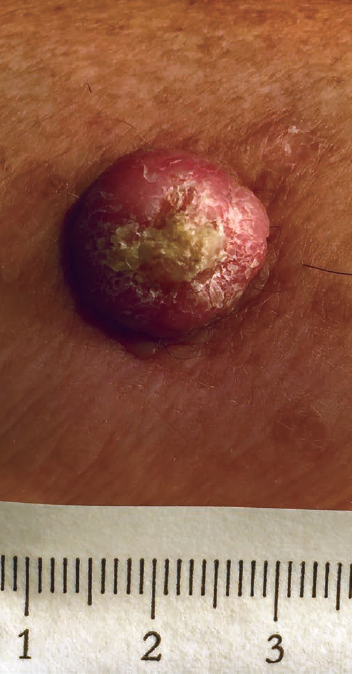
Physical examination revealed a 1.7 × 1.5-cm, red-yellow, raised, crusted nodule with central scaling on the lateral left upper arm. The lesion was tender upon palpation, without any discharge. The rest of the physical examination findings showed a fair-skinned man with areas of blotchy hyperpigmentation over sun-exposed areas.
Which one of the following is the most likely diagnosis?
- Basal cell carcinoma
- Squamous cell carcinoma
- Actinic keratosis
- Melanoma
- Seborrheic keratosis
Answer and discussion on next page.
Answer: Squamous Cell Carcinoma
An 85-year-old white male truck driver presented with a skin lesion on his left upper arm, approximately 5 cm above the elbow. He had noticed the lesion approximately 2 months ago as it slowly enlarged and became tender. The lesion often got caught in his sleeve and subsequently bled. He is a former smoker, and he has a history of renal cell carcinoma.
Physical examination revealed a 1.7 × 1.5-cm, red-yellow, raised, crusted nodule with central scaling on the lateral left upper arm. The lesion was tender upon palpation, without any discharge. The rest of the physical examination findings showed a fair-skinned man with areas of blotchy hyperpigmentation over sun-exposed areas.
Given the patient’s history and physical examination findings, this lesion was suspicious for squamous cell carcinoma (SCC).
The patient underwent a wide local excision that included 5-mm margins. Biopsy results confirmed the diagnosis of SCC, without involvement of the deep margins, thus requiring no further surgical or medical intervention. The patient tolerated the procedure well, and his case was followed up on a routine basis after the procedure.
Discussion
Cutaneous SCC is an invasive, primary cutaneous malignancy arising from keratinocytes of the skin and mucosal surfaces.1 It is caused by skin damage due to UV radiation exposure that leads to neoplastic transformation of epidermal keratinocytes. It is most commonly found on the back of the hands, the forearms, and other sun-exposed areas.
White patients with fair skin are at greatest risk. The most common risk factor is exposure to UV radiation. Other risk factors include tobacco exposure, hydrocarbons exposure, burns, chronic inflammation, chronic infections, immunosuppression, and a personal or family history of skin cancer. Men are affected at a 2 to 1 ratio.2 It is much more common in patients older than 60 years. It is the second most common skin cancer in the United States, with more than 100,000 new US cases of primary SCC diagnosed each year.1
Patients usually present with a nonhealing skin lesion on sun-exposed areas that is hard, scaly and usually bleeds with minimal trauma.2 Lesions may enlarge and become tender over a period of a few weeks to months. They may be over sun-damaged skin with freckled hyperpigmentation, atrophy, and telangiectasia. Typical lesions that go untreated develop into a firm red nodule, with a necrotic crusted lesion.1
Definitive diagnosis and staging are made via biopsy with histopathologic assessment. Treatment involves wide local excision that includes 4-6 mm of margins.3 At sites where tissue sparing is important, Mohs micrographic surgery may be utilized. Electrodessication, curettage, cryotherapy, and radiotherapy can also be used in certain situations. Once diagnosed and treated, it is important that patients have follow-up visits at regular intervals.
Nguyet-Cam V. Lam, MD, is the associate program director at the St. Luke’s Family Medicine Residency at St. Luke’s University Hospital in Bethlehem, Pennsylvania.
Neil B. Matalia, MD, was chief resident at the St. Luke’s Family Medicine Residency at St. Luke’s University Hospital in Bethlehem, Pennsylvania at the time this article was written.
References:
- Squamous cell carcinoma. In: Habif TP, Campbell JL Jr, Chapman MS, Dinulos JG, Zug KA. Skin Disease Diagnosis and Treatment. 3rd ed. Philadelphia, PA: Saunders Elsevier; 2011:483-487.
- Cutaneous squamous cell carcinoma. DynaMed Plus. https://www.dynamed.com/topics/dmp~AN~T116909/Cutaneous-squamous-cell-carcinoma. Updated October 28, 2016. Accessed November 8, 2016.
- Emer JJ, Waldorf HA. Squamous cell carcinoma. In: Lebwohl MG, Heymann WR, Berth-Jones J, Coulson I, eds. Treatment of Skin Disease: Comprehensive Therapeutic Strategies. 4th ed. Philadelphia, PA: Saunders Elsevier; 2014:718-722.