
Teenage Girl With Eye Drainage and "Bumps" on the Upper Eyelid

THE CASE: A 13-year-old girl reports that her right eye has been draining and uncomfortable for
the past several days. She is also concerned about several “bumps” on the upper lid of her left eye. She has had these bumps in the past, but they have always resolved spontaneously.
What you do suspect is the cause of the patient’s complaints?
•Hordeolum
•Conjunctivitis
•Blepharitis
•Chalazion
(Answer and discussion on next page.)
| Answer: Hordeolum |
DISCUSSION: This patient has a hordeolum, a localized inflammation of the eyelid also known as a stye, in the right eye, as well as multiple hordeola and a chalazion in the left eye. External hordeolum involves the eyelid margins; it results from obstruction and secondary infection of the Zeiss or Moll sebaceous glands. Internal hordeola, which are much less common, are caused by infection of the meibomian glands in the tarsal plate. About 90% to 95% of these infections are
attributable to Staphylococcus aureus.
Although many of the infections resolve spontaneously, some of them progress to form a chronic granulomatous lesion (chalazion).
Patients usually complain of localized painful swelling and eyelid edema, and they often have a history of recurrent hordeolum. A common secondary finding is injection of the conjunctiva. Hordeola are seen more frequently in patients with a history of seborrhea, chronic blepharitis, diabetes, or other chronic diseases.
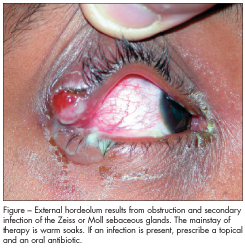 The mainstay of therapy for external hordeola is warm soaks. Topical antibiotics are frequently prescribed (Figure); however, they have not been shown to be effective unless secondary inflammation or infection is present. Systemic antibiotics are indicated only in the rare instance that bacteremia is suspected or if there are tender preauricular nodes. Surgical incision and drainage is usually warranted if the lesions do not respond to conservative treatment or if cosmetic deformity is present. This is best performed by an ophthalmologist or plastic surgeon.
The mainstay of therapy for external hordeola is warm soaks. Topical antibiotics are frequently prescribed (Figure); however, they have not been shown to be effective unless secondary inflammation or infection is present. Systemic antibiotics are indicated only in the rare instance that bacteremia is suspected or if there are tender preauricular nodes. Surgical incision and drainage is usually warranted if the lesions do not respond to conservative treatment or if cosmetic deformity is present. This is best performed by an ophthalmologist or plastic surgeon.
Outcome of this case. The hordeolum in our patient’s right eye had ulcerated, as evidenced by the
purulent drainage. She was treated with oral amoxicillin/potassium clavulanate and doxycycline, along with a topical corticosteroid/antibiotic ointment. Initial incision and drainage perfomed by a ophthalmologist was unsuccessful. On a follow-up visit, a local corticosteroid injection was administered and the amoxicillin/potassium clavulanate was discontinued. The topical medication was continued for 1 week and the doxycycline was continued for 4 weeks, at which time the patient’s lesion showed marked improvement.
Sorting through the differential. Conjunctivitis, an inflammation of the mucous membrane of the eye, is most commonly caused by a bacterial agent (such as Staphylococcus or Streptococcus) or a virus (such as herpes simplex or an adenovirus). Bacterial infections feature a mucopurulent discharge; with viral infections, the discharge is thin and watery. Eyelid edema and conjunctival injection are usually present. Treatment of bacterial infection consists of empiric antibiotic ointment or drops and cool compresses for symptomatic relief. Proper hygiene is mandatory to prevent spread of the infection.
Patients with blepharitis often complain of burning, inflammation, and irritation of the eyelids and eyelid margins. They may or may not have associated conjunctivitis. S aureus is usually the offending agent. Treatment involves antibiotic ointment and lid hygiene with a gentle detergent, such as baby shampoo.
Chalazia result from inflammation of the meibomian glands and present as painless, enlarging nodules of the eyelid (usually the upper one). The lesions are not infectious and are most commonly seen in adults between the ages of 30 and 50 years. Secondary injection of the conjunctiva may occur. If the chalazion is large enough, visual disturbances may result.
Chalazia may be associated with other processes, such as chronic blepharitis, hyperlipidemia, seborrhea, and acne rosacea. Conservative treatment with warm compresses usually is adequate. Antibiotics are not routinely recommended. Referral to a plastic surgeon or ophthalmologist is indicated for incision and drainage or corticosteroid injection if the chalazion has not resolved in several weeks.
FOR MORE INFORMATION:
• Durand M, Adamis A, Baker AS. Infections of the eyelid, lacrimal system, conjunctiva and cornea. Curr Clin Top Infect Dis. 1996;16:125-150.
• Rhee DJ, Pyfer MF, eds. The Wills Eye Manual. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 1999.