
Peer Reviewed
What is Responsible For This Girl's Cough, Fever, and Fatigue?
A 4-year-old girl with a history of 3 prior episodes of lobar pneumonia presented with a 2-day history of fever, with a temperature as high as 39°C. Eight days prior, the child had been referred for admission by her pediatrician for fever, leukocytosis (28,000 white blood cells/µL), and a left-sided infiltrate on chest radiographs (Figure 1). She had received 3 days of inpatient therapy with intravenous clindamycin to ensure lasting defervescence, waning leukocytosis, and falling levels of inflammatory markers; no oxygen requirement was noted throughout the hospitalization.
At the current presentation, the girl’s mother reported that the child had had worsening fatigue and a more frequent cough.
Both of the 2 additional previously documented pneumonias had involved the left lower lobe and had been treated in the outpatient setting, the first with ceftriaxone 6 months ago and the second with amoxicillin-clavulanate 4 weeks ago. No follow-up chest radiographs had been obtained between episodes to document interim resolution.
The child’s past medical history was significant for atopic dermatitis and allergic rhinitis but negative for asthma, wheezing episodes, nocturnal cough, frequent sinusitis, and recurrent otitis media. There was a remote family history of cystic fibrosis, but no direct blood relatives were affected.
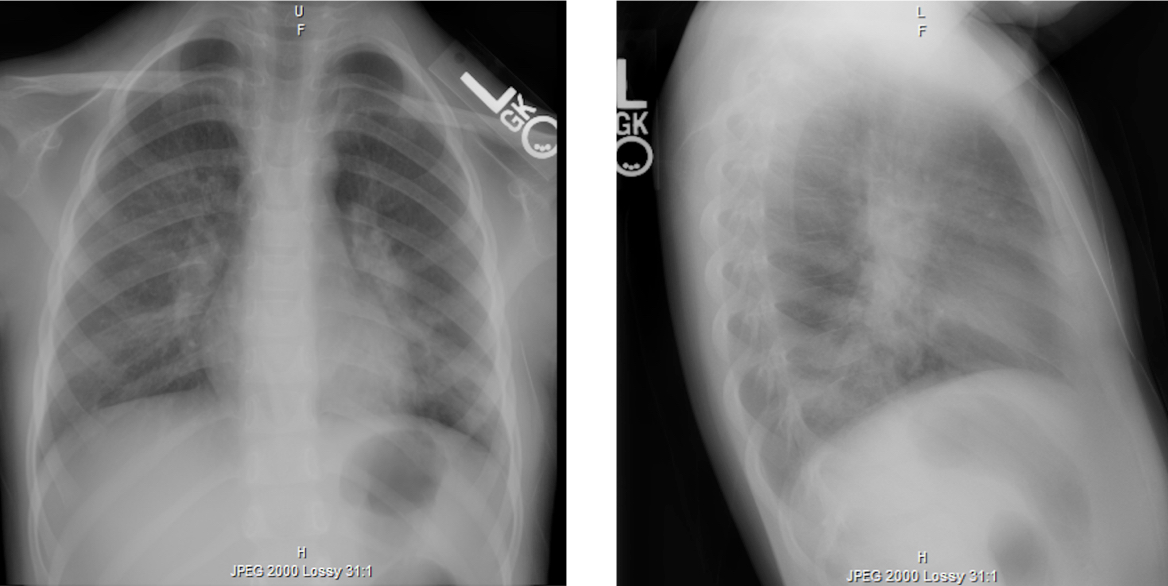
Figure 1. Chest radiographs demonstrating left lower-lobe opacity consistent with unilobar pneumonia.
Physical examination. At presentation, the patient was afebrile, with mild tachycardia. Otherwise, vital signs were stable. Physical examination findings were notable for a small, mobile, high right-anterior cervical-chain node and markedly diminished breath sounds in the left lung with egophony in her left axilla, as well as dullness to percussion.
Diagnostic tests. Laboratory test values were significant for a white blood cell count of 19,400/µL (76% neutrophils, 0% band forms), a platelet count of 543 × 103/µL, an erythrocyte sedimentation rate of 35 mm/h, and a C-reactive protein level greater than 9 mg/L.
These findings, along with recurrent fever and fatigue in the context of frequent, recent pneumonias, prompted concern for possible empyema, pleural effusion, or pulmonary sequestration. Chest computed tomography (CT) with contrast demonstrated dense, organized consolidation and obliteration of the associated lobar bronchus but no systemic arterial supply or pleural fluid (Figure 2).
Serum immunoglobulin levels were unremarkable, and test results for Mycoplasma pneumoniae immunoglobulin M were negative. The child was transferred to a tertiary care center for diagnostic bronchoscopy, where a tenacious mucus plug of the associated lobar bronchus was extracted as the likely source of recurrent obstruction and subsequent pneumonia.
Five months later, the family reported that the child had had no further respiratory illnesses. Pulmonary function testing had been deferred due to the patient’s age, and genetic testing results were negative for mutation of the cystic fibrosis transmembrane conductance regulator gene (CFTR).
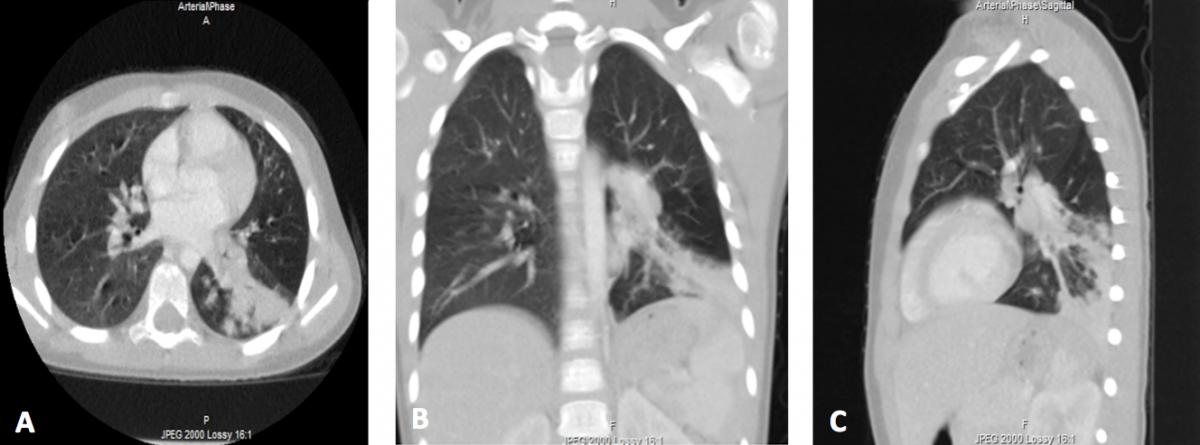
Figure 2. Axial (A), coronal (B), and sagittal (C) contrast-enhanced CT images demonstrating left lower-lobe bronchial obstruction.
Discussion: Recurrent pneumonia is characterized by more than 2 episodes of pneumonia in 1 year or at least 3 episodes in any time period, with radiographic evidence of resolution between events.1 Endobronchial obstruction, extraluminal compression, and respiratory tract structural malformations should be considered in a child presenting with recurrent pneumonia of unilobar origin,2 as demonstrated in our case. Inhaled foreign bodies and endobronchial tumors can cause intraluminal obstruction, while enlarged lymph nodes, parenchymal neoplasms, and vascular rings may cause extrinsic bronchial compression.3 Anatomic defects, namely congenital pulmonary adenomatoid malformations undiagnosed in utero, bronchogenic cysts, pulmonary sequestrations, bronchomalacia, and bronchial stenosis must also be considered.2 Bronchoscopy and chest CT can be particularly helpful in the workup of recurrent pneumonia, while an aortogram may facilitate diagnosis of pulmonary sequestration.3
Additionally, aspiration pneumonia secondary to oropharyngeal incoordination, gastroesophageal reflux, congenital and acquired immune disorders, and infectious diseases leading to postinfective bronchiectasis should be ruled out, particularly in children presenting with recurrent multilobar pneumonia.3 Interestingly, refractory Mycoplasma infections have been linked to bronchial plugging.4 Cystic fibrosis, asthma, and ciliary dysfunction are also important causes of recurrent pneumonia and chronic lung infections in children, since they can cause significant mucus plugging in the airways.5 While our patient was noted to have a substantial bronchial mucus plug in the context of recurrent pneumonia, her case is unique in that she had no substantiated history of cystic fibrosis, asthma, or ciliopathy.
References:
- Wald ER. Recurrent and nonresolving pneumonia in children. Semin Respir Infect. 1993;8(1):46-58.
- Panitch HB. Evaluation of recurrent pneumonia. Pediatr Infect Dis J. 2005;24(3):265-266.
- Yousif TI, Elnazir B. Approach to a child with recurrent pneumonia. Sudan J Paediatr. 2015;15(2):71-77.
- Xu Q, Zhang L, Hao C, et al. Prediction of bronchial mucus plugs formation in patients with refractory Mycoplasma pneumoniae pneumonia. J Trop Pediatr. 2017;63(2):148-154.
- Bickel S, Wiese T, O’Hagan A, Mortin R, Eid NS. Recurrent pneumonia as a manifestation of severe mucus plugging in an asthmatic [abstract]. Am J Respir Crit Care Med. 2015;191:A5488.