
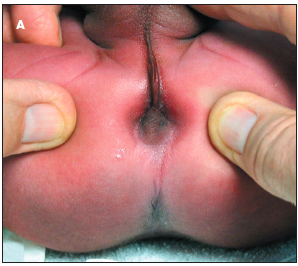
 During their physical examination of this infant who had been born at term via cesarean section, Richard W. Hartmann, Jr, MD, and J. Christiane Salansky, MD, of Halifax Medical Center, Daytona Beach, Fla, found no evidence of an external anal opening (A). A soft bulge was present at the anal site, and the external sphincter was palpable. The median raphe was thick; a drop of meconium was noted on the surface of the perineum midway from the anus to the base of the scrotum (B). The remainder of the examination findings were normal.
During their physical examination of this infant who had been born at term via cesarean section, Richard W. Hartmann, Jr, MD, and J. Christiane Salansky, MD, of Halifax Medical Center, Daytona Beach, Fla, found no evidence of an external anal opening (A). A soft bulge was present at the anal site, and the external sphincter was palpable. The median raphe was thick; a drop of meconium was noted on the surface of the perineum midway from the anus to the base of the scrotum (B). The remainder of the examination findings were normal.
Abnormalities of anorectal development are classified anatomically as high, intermediate, and low. The pu-borectalis muscle sling (part of the levator ani muscle group) is the cutoff for the classification. A fistula is present in 95% of patients with an anorectal abnormality.1
Male infants with high and intermediate defects have a fistula from the rectum to the urinary tract, often into the prostatic urethra. In female infants with high and intermediate defects, the fistula opens into the vagina. Meconium noted in the urine or leaking from the vagina suggests a high or intermediate defect.2 
In infants with a low anorectal malformation, such as this newborn, the fistula is usually anocutaneous.3 The subepithelial tract travels the median perineal raphe and might exit anywhere up to the base of the scrotum in a male infant and at or near the vestibule of the vulva in a female infant. Meconium in amniotic fluid does not rule out the presence of an anorectal malformation; the fistula allows the meconium to pass into the fluid.
Diagnosis requires close inspection and palpation of the anus and perineum. A fistula may be difficult to detect. Meconium can usually be milked along the thick median raphe until the point of exit is visualized.
The frequency of additional congenital malformations varies from 40% to 70%.4 High and intermediate defects are more likely to have associated malformations, of which vertebral and renal lesions are the most common.
Anorectal malformations are more common in patients with VACTERL association (vertebral, anal, cardiac, tracheoesophageal, renal, and limb malformations), trisomy 21, Currarino triad, posterior urethral valves, and spinal dysraphism.5-7 Isolated imperforate anus in monozygotic twins has been reported.8
Surgical repair of anorectal malformations is required; the outcome is better for patients with a low anomaly. The abnormality in this infant was successfully repaired.