
Case 1:
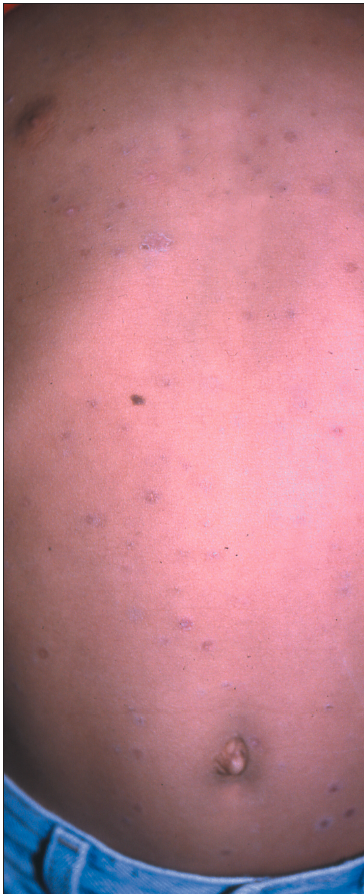 For several weeks, a 6-year-old girl has had a worsening mildly pruritic rash on the trunk. She has a history of seasonal allergies. The family has had a cat and a dog in the house for a number of years.
For several weeks, a 6-year-old girl has had a worsening mildly pruritic rash on the trunk. She has a history of seasonal allergies. The family has had a cat and a dog in the house for a number of years.
What do you suspect?
A. Tinea corporis.
B. Pityriasis rosea.
C. Nummular eczema.
D. Asteatotic eczema.
E. Lichen simplex chronicus.
F. Contact dermatitis.

Case 1: This patient has pityriasis rosea, B, which is more common in children and in young adults than in older adults. This self-limited eruption typically presents with oval macules that are more or less pruritic. The condition usually runs its course over several weeks; topical corticosteroid creams relieve the symptoms. Tinea corporis, nummular eczema, asteatotic eczema, and contact dermatitis do not present with multiple discrete lesions as small as these. Lichen simplex chronicus is unusual in children and does not feature such numerous lesions.
It is unlikely that a dermatophyte infection would produce so many lesions so quickly--so the family pets cannot be blamed.
Case 2:
 A 10-year-old girl who plays soccer at school has had pruritic papules on her elbows for several weeks. She has not been exposed to any new detergents or new clothing. Her family has a cat and a dog. No one else in the family has similar lesions, although her brother has seasonal allergies.
A 10-year-old girl who plays soccer at school has had pruritic papules on her elbows for several weeks. She has not been exposed to any new detergents or new clothing. Her family has a cat and a dog. No one else in the family has similar lesions, although her brother has seasonal allergies.
What type of eruption is this?
A. Scabies.
B. Psoriasis.
C. Atopic dermatitis.
D. Lichen spinulosus.
E. Granuloma annulare.
Case 2: The patient has atopic dermatitis, C. This condition generally presents in children aged 2 to 12 years as pruritic papules in the flexural areas. The rash can be controlled with moisturizers and low-potency topical corticosteroids.
Scabies would generally be more widespread after a few weeks. Psoriasis is more scaly and patchy. Lichen spinulosus may erupt on the elbows in atopic patients, but it typically is asymptomatic. Granuloma annulare is also asymptomatic.
It is unlikely that a dermatophyte infection would produce multiple discrete pruritic papules like these on the elbows. Thus, the family pets are not a likely source.
Case 3:
A 12-year-old boy presents with a symmetric pruritic rash on his arms and legs that has coincided with the onset of his seasonal allergies. He has taken montelukast( and cetirizine for years. He participates in sports year-round and sometimes takes more than 1 shower a day. The family owns a dog and a ferret.
 What do you suspect?
What do you suspect?
A. Adverse drug reaction.
B. Contact dermatitis.
C. Atopic dermatitis flare.
D. Psoriasis.
E. Tinea corporis.
Case 3: This patient has an atopic dermatitis flare, C. The synchronous occurrence of atopic dermatitis and a respiratory condition is seen occasionally. The patient's dermatitis was exacerbated by excessive bathing, a habit common among adolescents. His condition improved with a regimen of fewer showers, moisturizers, and a moderately potent topical corticosteroid.
Neither montelukast nor cetirizine is likely to produce a cutaneous drug reaction such as the one seen here. The pattern and location of the patient's rash are not typical of contact dermatitis. Psoriasis is scalier than this patient's rash. It is unlikely that a dermatophyte eruption would arise so quickly and be so extensive.
Dermatophytic infection is not usually this extensive unless the patient is immunocompromised. Thus, the patient's dog and ferret are off the hook.
Case 4:
An 8-year-old girl presents with a pruritic rash of several weeks' duration in the antecubital fossae. There is a family history of seasonal allergies, and the family has a 2-year-old dog.
Can you identify the rash?
A. Candidiasis.
B. Dermatophyte infection.
C. Atopic dermatitis.
D. Contact dermatitis.
E. Impetigo.
 Case 4: The results of a potassium hydroxide( evaluation were negative, which supported the diagnosis of atopic dermatitis, C. This condition, known colloquially as "the itch that rashes," preferentially affects large flexural surfaces, such as the antecubital and popliteal fossae.
Case 4: The results of a potassium hydroxide( evaluation were negative, which supported the diagnosis of atopic dermatitis, C. This condition, known colloquially as "the itch that rashes," preferentially affects large flexural surfaces, such as the antecubital and popliteal fossae.
It is highly unlikely that candidiasis or a dermatophyte infection would be bilateral. The antecubital fossae are not a typical location for contact dermatitis. Impetigo features oozing and crusting.