

THE CASE: A 21-month-old previously healthy child is brought to the pediatrician's office because of increasingly labored breathing that began the night before. The father reports that the child has had fever, congestion, nonproductive cough, and irritability for 2 days and that she is slightly hoarse. Oral intake has decreased, but there is no drooling or dysphagia. Temperature is 40.3°C (104.6°F); heart rate, 190 beats per minute; respiration rate, 32 breaths per minute; oxygen saturation, 93% on room air.
The patient is in mild respiratory distress, with inspiratory stridor and supraclavicular retractions. The posterior oropharynx is symmetric and free of masses, but there is a mass in the right lateral neck. There is no rash, and results of the neurologic examination are normal. Because of concern about her respiratory status, the child is sent to the emergency department.
Which of the following conditions do you suspect?
• Cystic hygroma
• Epiglottitis
• Round pneumonia
• Foreign-body aspiration
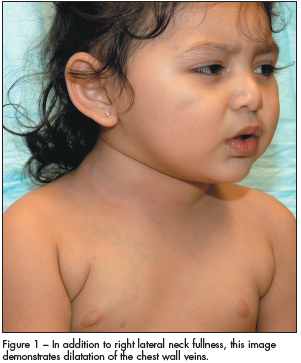 DISCUSSION: In addition to the lateral neck mass, physicians in the emergency department noted dilated superficial vessels on the right anterior chest wall (Figure 1). A chest radiograph demonstrated a large density in the right upper lobe with a mediastinal shift to the left side (Figure 2).
DISCUSSION: In addition to the lateral neck mass, physicians in the emergency department noted dilated superficial vessels on the right anterior chest wall (Figure 1). A chest radiograph demonstrated a large density in the right upper lobe with a mediastinal shift to the left side (Figure 2).
Antibiotic therapy was started. Because of increasing respiratory distress, the child underwent elective intubation and was admitted to the pediatric ICU. A 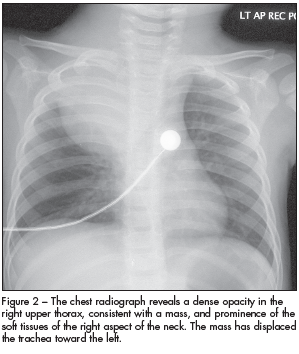 CT scan of the neck and chest revealed a hypodense fluid collection with multiple septa extending from the retropharyngeal space into the mediastinum. There was significant compression of the trachea and thoracic vasculature. After the otolaryngologist and thoracic surgeon were consulted, the child underwent surgery. An infected cystic hygroma was found and excised.
CT scan of the neck and chest revealed a hypodense fluid collection with multiple septa extending from the retropharyngeal space into the mediastinum. There was significant compression of the trachea and thoracic vasculature. After the otolaryngologist and thoracic surgeon were consulted, the child underwent surgery. An infected cystic hygroma was found and excised.
A cystic hygroma is a benign structure that arises from a developmental lymphatic abnormality. The resulting collection of obstructed lymphatic channels produces nontender, fluctuant cystic masses that often extend into the soft tissues. They are usually identified before a child is 2 years old and are most commonly found in the neck.
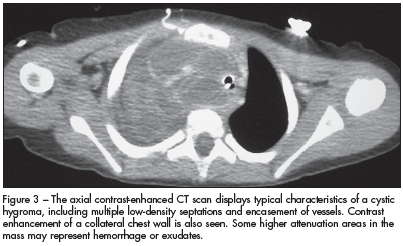
In the presence of trauma or an upper respiratory tract infection, a cystic hygroma often becomes infected and grows rapidly, a process that produces fever and pain. Infiltration of the mass into the floor of the mouth, base of the tongue, epiglottis, or mediastinum can compromise the airway. This rapid enlargement of the mass secondary to infection accounts for the clinical signs and symptoms. In addition, our patient's clinical findings were consistent with superior vena cava syndrome (venous congestion, dysphonia, dyspnea, and dilated chest wall veins), which eventuated from thoracic compression of the hygroma (Figure 3).
The diagnosis of an infected cystic hygroma can be difficult because other processes--including retropharyngeal abscesses and infected branchial cleft cysts--also present with a neck mass, fever, and stridor. In many cases, advanced imaging is necessary to confirm the diagnosis. CT or MRI of a cystic hygroma typically reveals a multiloculated cystic mass. CT can delineate the size of the mass, although MRI more reliably identifies extension into the soft tissues, particularly neurovascular structures.
Airway management is critical because of the rapid growth of the mass, particularly when stridor, tracheal deviation, and voice changes are present. Surgical excision is considered the treatment of choice, although other options, such as sclerotherapy, interferon treatments, and carbon dioxide laser ablation, have been used with some success.
 The bacterial infection epiglottitis may present with fever, dyspnea, and stridor. Other symptoms include dysphagia, dysphonia, and pharyngitis. Patients often drool and can be found leaning forward with the mouth open and neck extended in the "tripod" position. Unlike the stridor of cystic hygroma, stridor in epiglottitis results from upper airway edema and obstruction, not from external mass effect. A lateral neck plain film can be diagnostic if it shows thickened aryepiglottic folds or a dilated hypopharynx with classic enlargement of the epiglottis (known as the "thumbprint" sign). However, direct visualization more sensitively confirms the diagnosis.
The bacterial infection epiglottitis may present with fever, dyspnea, and stridor. Other symptoms include dysphagia, dysphonia, and pharyngitis. Patients often drool and can be found leaning forward with the mouth open and neck extended in the "tripod" position. Unlike the stridor of cystic hygroma, stridor in epiglottitis results from upper airway edema and obstruction, not from external mass effect. A lateral neck plain film can be diagnostic if it shows thickened aryepiglottic folds or a dilated hypopharynx with classic enlargement of the epiglottis (known as the "thumbprint" sign). However, direct visualization more sensitively confirms the diagnosis.
The most common causative organism has been Haemophilus influenzae, although the incidence of H influenzae infection has been declining with widespread administration of the H influenzae type B vaccine. Definitive treatment involves parenteral antibiotics. A critical step in the management of patients with epiglottitis is avoidance of excessive agitation or anxiety-provoking measures, because these may further compromise an already impaired airway. Ideally, oxygen is delivered in a non-threatening manner and direct laryngoscopy is performed in a controlled setting in which a surgical airway can be provided if necessary.
Round pneumonia refers to a radiographic finding commonly seen in children with pneumonia. Chest radiography reveals a round infiltrate that is sometimes confused with a solitary pulmonary nodule. The lesion usually manifests in the posterior portion of the lower lobe. The round appearance of the infiltrate is thought to result from centrifugal spread of the consolidation process. The most common infectious agent is Streptococcus pneumoniae, although other organisms--including H influenzae, Klebsiella, and Mycobacterium tuberculosis--have been identified. Neoplasms must be considered in the differential diagnosis. In adults, round pneumonia is most frequently seen in immunocompromised patients and is often attributable to Aspergillus infection.
The clinical presentation of round pneumonia is similar to that of pneumonia. Signs and symptoms include cough, fever, chest pain, and dyspnea. Antibiotics are started, and the radiographic findings should begin to resolve within 1 week.
Foreign-body aspiration is most commonly encountered in children, especially those younger than 3 years. Patients may present after a choking episode with the sudden onset of symptoms or after a delayed period. Nuts are the most commonly aspirated foreign bodies. The clinical presentation may be mild; sometimes cough is the only finding. At the other extreme, the child may be in obvious respiratory distress, with nasal flaring, retractions, decreased breath sounds, stridor, wheezing, cyanosis, or respiratory failure. Initial misdiagnoses of reactive airway disease, bronchitis, or infection are frequent. Patients are normally afebrile unless there has been a delay in diagnosis and a secondary process (such as infection or inflammation) has begun.
Foreign bodies may obstruct any portion of the airway but most often lodge in the right mainstem bronchus of the lung. Although the foreign body occasionally appears on radiography, most aspirated objects are radiolucent. In these cases, the radiograph may appear normal, but hyperinflation or atelectasis provides subtle evidence of an aspirated object. Bronchoscopy is often required for identification and removal of the object.