The conventional method of placing an umbilical artery catheter in neonates involves cutting the cord approximately 1 cm above the skin/cord junction. The cord stump is then held steady with 2 or more hemostats while the vessels are dilated and cannulated.1-3 Although this method has been successfully employed by generations of pediatricians, the technique requires considerable practice to master.
hemostats while the vessels are dilated and cannulated.1-3 Although this method has been successfully employed by generations of pediatricians, the technique requires considerable practice to master.
Most cases of unsuccessful catheter insertion result from awkward positioning and handling of the umbilical stump, which tends to retract into the abdomen. It is nearly impossible to get a firm grasp, which makes it difficult to visualize umbilical vessels. This results in the creation of false tracts during vessel dilation and/or perforation of the vessel when attempts are made to insert the catheter.
 We have experimented with several small modifications of standard catheter insertion techniques that can make it easier to insert an umbilical artery line. Our technique facilitates successful line placement.
We have experimented with several small modifications of standard catheter insertion techniques that can make it easier to insert an umbilical artery line. Our technique facilitates successful line placement.
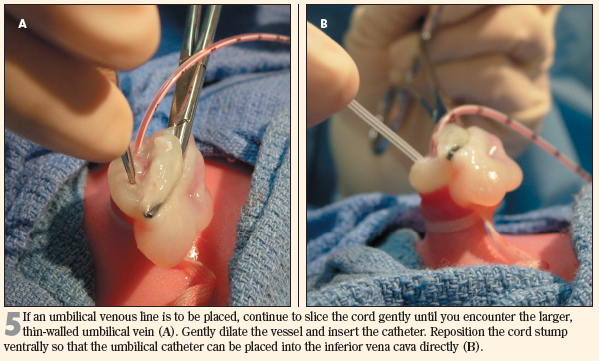
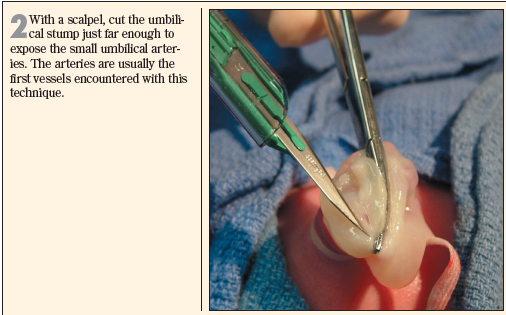
Professional cooks use the term "butterfly" to describe the partial cutting of a fillet or other food item in a manner that increases the surface area exposed to heat.We advocate a butterfly technique in which the umbilical cord is partially sliced so that the umbilical artery is exposed. When the upper flap of the cord is folded over, the umbilical vessels are pulled upward and outward. They are easily identified and are fixed in place by the tension placed on the folded cord flap.
Mechanical advantage is maximized because: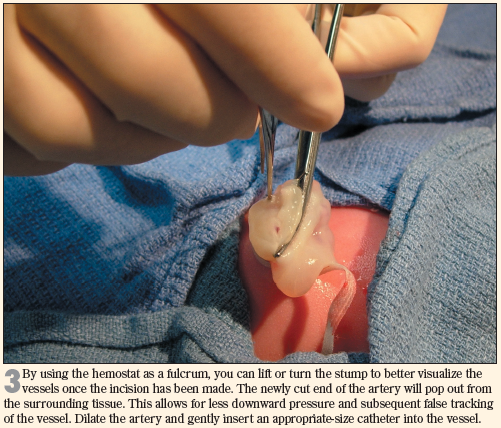
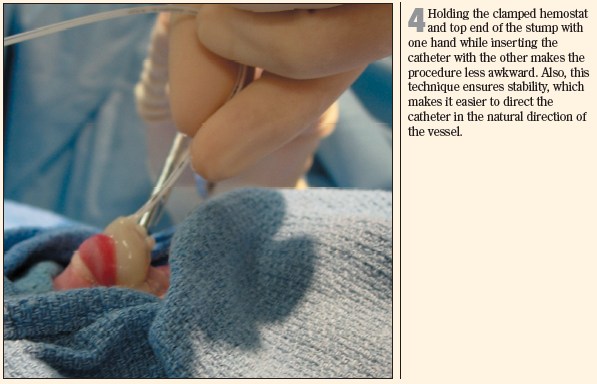
• The cord stump is the fulcrum.
• The hemostat is the lever.
• The directionality of catheter insertion is the inclined plane.
Practitioners at all levels of experience have had success with this technique.