
ABSTRACT: Recurrent headaches that are accompanied by the need to rest during attacks, a family history of migraines, and benign physical findings are migraine until proved otherwise. It is essential that teachers and the school nurse allow the child access to medication at the first twinge of headache and to rest for a short time before returning to class. The worst strategy is to send the child back to class immediately without medicine because the headache is “not so bad.”
 Figure - This self-portrait was drawn by a child who suffers from migraine headaches. |
In most children, migraine manifests with severe bilateral pain, nausea and/or vomiting, and photophobia or phonophobia (Figure). While this presentation can be alarming—particularly for parents whose worst fear is that their child has a brain tumor—it is actually classic for pediatric migraine.
This article focuses on making the diagnosis, addressing stress and other trigger factors--and helping school staff understand the importance of early intervention when a migraine develops while a child is at school. For details on treating acute attacks and on preventing recurrences, the reader is referred to several excellent articles on this topic.1-4
CLUES TO THE DIAGNOSIS
Headache pattern. Pediatric headaches occur in four distinctive patterns5:
•Acute.
•Acute recurrent.
•Chronic progressive.
•Chronic nonprogressive.
Most headaches that fit the acute recurrent pattern are migraines. Suspect this diagnosis when a child or teenager has acute severe recurrent headaches that are accompanied by autonomic symptoms (Table 1).
Symptoms that mimic migraine. Migraine is underdiagnosed--and misdiagnosed--frequently as "tension" headache. When migraine presents with neck pain, the diagnosis is often tension headache. Remember, however, that headache with autonomic symptoms and an acute recurrent pattern is migraine--not tension headache. The location of the pain is not a helpful diagnostic clue.6
Migraine is also often misdiagnosed as "sinus" headache. Because the second branch of the trigeminal nerve innervates the nose, eyes, and maxillary sinus areas, lacrimation, rhinorrhea, and/or sinus tenderness may occur during an acute migraine episode. If there are autonomic symptoms and the pattern is acute and recurrent, however, the diagnosis is migraine--not sinus disease. Sinus disease presents with fever, cough, and halitosis; symptoms do not resolve and then recur like migraines.7,8 A patient with chronic sinusitis may have chronic headache, but this topic transcends the scope of this article.
Prodromic symptoms. A migraine attack may be preceded by such symptoms as sluggishness and hunger. Patients may have difficulty with words and may experience a feeling of doom similar to that experienced by some patients with seizures.
Aura. In most children, migraine occurs without an aura.9 When present, migraine aura is usually stereotypical. Wavy lines start peripherally and move across the visual field, usually sparing the midline. Headache usually begins about 30 minutes after the onset of these "fortification spectra."
Other autonomic symptoms. Children with migraine commonly experience dizziness, light-headedness, pallor, or purple "bags" around the eyes. Ask the child's mother whether she can usually tell if her child has a headache just by looking at him.
Migraineurs have a heightened sensitivity to flickering lights. They tend to startle easily and have more sensitive skin between headache attacks.10 Gastroparesis may be present, even when a migraineur is not experiencing an attack.11
Headache pain. In children, migraine pain usually lasts between 1 and 72 hours (shorter than in adults) and the pain is more often bilateral than in older persons.9 The time of day in which headache pain occurs is not a particularly helpful diagnostic clue in pediatric migraine.
Other diagnostic clues. To gauge the degree of disability during an attack, ask the patient whether he or she is able to run up and down the stairs during a headache. The inability to exercise during a headache supports the diagnosis of migraine. During an attack, a child or adolescent with migraine will typically retreat to a dark, quiet place and lie down in an attempt to decrease external stimulation.
HISTORY AND PHYSICAL EXAMINATION
How have the headaches affected the patient and family members? Objective measures include the number of days of school missed. Other markers of disability include family (dys)function, curtailment of after-school activities, and a general description of what happens at home when the patient gets a headache. The Peds-MIDAS Scale offers an objective measure of disability that can be followed over time.12,13
Find out the number of days the child is in school but not performing at full capacity because of headaches. This information offers a glimpse at the difference between actual and potential performance in school.
The physical examination ensures that nothing important is missed and reassures both clinician and patient. Patients need to be fully undressed and examined in a gown. (The presence of café au lait spots or scoliosis may suggest intracranial pathology.) Vital signs may reveal undiagnosed hypertension as well as Cushing triad. The examination is standard, and a thorough neurological examination is indicated.
Fortunately, there are usually few physical surprises. If a child's clinical story is consistent with migraine and if the physical findings are normal, no further workup is necessary.14,15
HEADACHE TRIGGERS
A long list of migraine triggers has been implicated.16 These can be mitigated somewhat if the child eats, exercises, and sleeps regularly. School is a significant migraine trigger. School stressors include waking up very early, worrying about grades or social issues, undiagnosed learning disabilities, and parental pressure.17,18 For the "stressed-out kid" with a "full plate" of school and extracurricular activities, it may help to give permission to lighten up the child's load a bit. In many children, migraines go into "remission" during the summer, and begin again once school is under way.
The role of diet in pediatric headache remains controversial.19,20 However, patients may benefit by avoiding such triggers as caffeine, monosodium glutamate, chocolate, cheese, and sulfites (Table 2).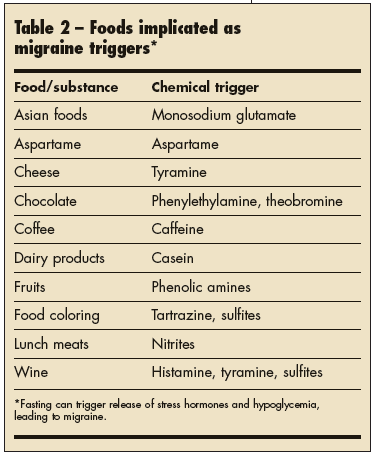
WHEN A MIGRAINE OCCURS AT SCHOOL
In the school setting, it is often difficult for a child to find a dark, quiet place in which to lie down. Triptan medications can be taken at school at the first signs of headache. These agents allow the child to resume school activities (see "Triptans: What Role in Pediatric Migraine?").
The lesson for the child and the school nurse is to aggressively treat headache at the first twinge. The worst strategy is to send the child back to class immediately without medicine because the headache is "not so bad." For migraineurs, the prescribed medication should be taken even during milder attacks.
It is essential that teachers and the school nurse allow the child access to medication at the first twinge of headache, and to rest for a short time before returning to class.21 A note from the clinician to the school staff can be particularly helpful in enlisting the school's cooperation. The note should stress the importance of early intervention and the need for the youngster to take his medication immediately.
Dehydration is a headache trigger for many young migraineurs. It is important for teachers to understand the need for the child to drink at his desk--and to grant bathroom privileges as needed (despite the potential for classroom disruption).
Certain teachers drop student's grades for attendance reasons. This must be discouraged for migraine patients. The stress of artificial grade dropping may exacerbate migraines. Rather, a liberal makeup policy for missed days gives the migraineur some control and assurance that he will not be punished for days when no work can be done. Help teachers and administrators understand that while a child is in the throes of a migraine, it is impossible to concentrate on school work.
The biggest mistake is to allow a pediatric migraineur to stop attending school because of headaches.22 Although school may be stressful, it is a child's job. Once a child is out of school, it is extremely hard to get him back in school.
The doctor and school staff can develop a partial attendance program (eg, in which the school day starts a little later than usual and accommodations are made when a child is absent). Such a program is preferable to home school programs. Many children feel isolated and defeated when told they cannot return to school. On the other hand, some youngsters with migraine relish the idea of staying home. Obviously, avoidance is not the answer.
THE BOTTOM LINE
Headaches that follow an acute recurrent pattern and that are accompanied by autonomic symptoms, the need to rest during attacks, a family history of migraines, and benign physical findings are migraines until proved otherwise. When a migraine develops at school, a triptan should be taken at the first sign of headache.