
Pathophysiology of Diabetes in the Elderly
This article is the first in a continuing series on diabetes in the elderly. The series will discuss such topics as quality improvement efforts, the role of exercise and dietary supplements in the management of diabetes, treatment of diabetes with oral and parenteral agents, as well as microvascular and macrovascular complications of diabetes. The second article in the series, “Quality Improvement in the Diagnosis and Management of Diabetes Mellitus in Older Adults,” will be published in the next issue of the Journal.
Diabetes in the elderly is unique. The pathophysiology of this condition is different in the elderly, and, as a consequence, the therapeutic approach should be different.1
There are a number of reasons why the incidence and prevalence of diabetes increases with age. There is clearly a genetic predisposition to this disease.2 If you have a family history of diabetes, you are much more likely to develop diabetes as you age, although the specific genes responsible have not been identified. Diabetes is clearly more common in older people from certain ethnic groups than others, which further supports a genetic predisposition.3
There are also a number of age-related changes in carbohydrate metabolism that allow a genetic predisposition for diabetes to become manifest in older people. These include progressive detriments in glucose-induced insulin secretion (which may be due, in part, to a decreased beta cell response to the incretin hormones GIP and GLP-1) and resistance to insulin-mediated glucose disposal.4-6
It is abundantly clear that various environmental and lifestyle factors can also increase the likelihood that a genetically susceptible individual will develop diabetes in old age.1,7 Many older people have co-existing illnesses and take multiple drugs that can adversely impact glucose metabolism. There is an age-related increase in obesity, particularly central obesity, and a reduction in physical activity, both of which can be associated with abnormal glucose metabolism. It is clear that diabetes is more likely to develop in older people who have a diet that is high in saturated fats and simple sugars and low in complex carbohydrates. Moderate alcohol consumption appears to be protective against diabetes, at least in women, whereas greater intake of dietary iron may be associated with an increased risk of diabetes in the elderly. It has been suggested that deficiencies of trace elements such as zinc and chromium and vitamins such as C and E may contribute to the development of diabetes in the elderly, but the data in this regard are unclear. The above information suggests that lifestyle modifications might be of value in the diabetes prevention in older people. In fact, the Diabetes Prevention Program found that modifications of diet and activity were more effective in older people than in younger patients in preventing the development of diabetes.8
The presence of inflammation, as evidenced by increased levels of proinflammatory cytokines such as C-reactive protein and tumor necrosis factor-alpha, is associated with an increased incidence of diabetes in the elderly.9 On the other hand, higher levels of adiponectin (an adipocytokine that increases insulin sensitivity) are associated with a reduced incidence of diabetes. Lower testosterone levels in men and higher testosterone levels in women also appear to be associated with an increased incidence of diabetes.
Metabolic Alterations
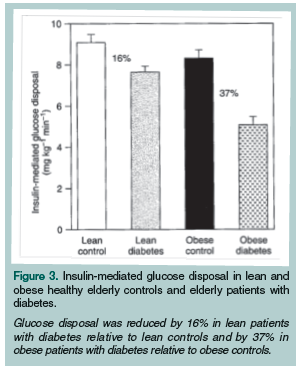
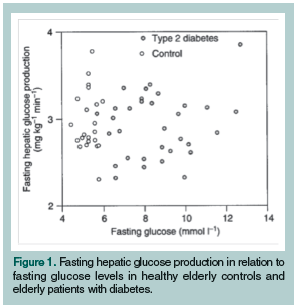 The metabolic abnormalities in middle-aged patients with type 2 diabetes have been extensively studied.2,10 In both lean and obese subjects, there is an increase in fasting hepatic glucose production, a reduction in glucose-induced insulin release, and a marked impairment in insulin-mediated glucose disposal. Recently, we and others have characterized the metabolic alterations in older people with diabetes and have demonstrated a different metabolic profile from younger patients with this disease.11-14 In the elderly, fasting hepatic glucose production is not increased (Figure 1). Obese older subjects, like obese younger subjects, have a marked impairment in insulin-mediated glucose disposal, but unlike younger subjects they have relatively preserved glucose-induced insulin secretion (Figures 2 and 3). Lean elderly subjects have a marked impairment in insulin secretion but relatively preserved insulin sensitivity. In summary, the primary metabolic defect in obese older people with diabetes is insulin resistance, whereas the principal defect in lean subjects is a reduction in glucose-induced insulin release. Therefore, in lean older subjects, the main initial approach should be to administer insulin or give insulin secretogogues. Obese patients should be treated initially with drugs that improve insulin sensitivity, such as metformin.
The metabolic abnormalities in middle-aged patients with type 2 diabetes have been extensively studied.2,10 In both lean and obese subjects, there is an increase in fasting hepatic glucose production, a reduction in glucose-induced insulin release, and a marked impairment in insulin-mediated glucose disposal. Recently, we and others have characterized the metabolic alterations in older people with diabetes and have demonstrated a different metabolic profile from younger patients with this disease.11-14 In the elderly, fasting hepatic glucose production is not increased (Figure 1). Obese older subjects, like obese younger subjects, have a marked impairment in insulin-mediated glucose disposal, but unlike younger subjects they have relatively preserved glucose-induced insulin secretion (Figures 2 and 3). Lean elderly subjects have a marked impairment in insulin secretion but relatively preserved insulin sensitivity. In summary, the primary metabolic defect in obese older people with diabetes is insulin resistance, whereas the principal defect in lean subjects is a reduction in glucose-induced insulin release. Therefore, in lean older subjects, the main initial approach should be to administer insulin or give insulin secretogogues. Obese patients should be treated initially with drugs that improve insulin sensitivity, such as metformin.
 It has also been shown that insulin-mediated vasodilatation, which accounts for over 30% of normal glucose disposal, is impaired in obese insulin-resistant older patients with diabetes.7 This suggests that drugs that enhance muscle blood flow may be beneficial, and indeed angiotensin-converting enzyme (ACE) inhibitors have been demonstrated to improve insulin sensitivity in these patients.1
It has also been shown that insulin-mediated vasodilatation, which accounts for over 30% of normal glucose disposal, is impaired in obese insulin-resistant older patients with diabetes.7 This suggests that drugs that enhance muscle blood flow may be beneficial, and indeed angiotensin-converting enzyme (ACE) inhibitors have been demonstrated to improve insulin sensitivity in these patients.1
It has been known for a long time that autoimmune phenomena play a major role in the beta cell failure that occurs in patients with type 1 diabetes.15 It is also increasingly recognized that there is a subset of patients with type 2 diabetes who have islet cell antibodies, and these patients are considered to have latent autoimmune diabetes in adults (LADA). It is unclear at the present time what percentage of insulin-dependent older people with diabetes have LADA. In general, these patients are lean subjects who fail oral agents and require insulin therapy early in the course of their disease. In the future it may be recommended that autoimmune parameters be measured at diagnosis in elderly patients with type 2 diabetes, since there is emerging evidence that early insulin therapy and antigen-specific immunomodulation may delay the time to insulin therapy in some of these patients. Further investigations will be needed to prove this hypothesis.
 It has been known for a long time that the insulin response to oral glucose is greater than intravenous glucose, and this is known as the incretin effect. The hormones responsible for this effect are GIP and GLP-1. The beta cell of older people with diabetes does not respond to GIP, but the responses to exogenous GLP-1 are preserved.1,7 Preliminary data suggest that the dipeptidyl peptidase 4 (DP4) inhibitors, which prevent the breakdown of endogenous GLP-1, or long-acting GLP-1 analogues such as exenatide maintain their efficacy in older patients and should be considered as appropriate therapeutic interventions in this age group.
It has been known for a long time that the insulin response to oral glucose is greater than intravenous glucose, and this is known as the incretin effect. The hormones responsible for this effect are GIP and GLP-1. The beta cell of older people with diabetes does not respond to GIP, but the responses to exogenous GLP-1 are preserved.1,7 Preliminary data suggest that the dipeptidyl peptidase 4 (DP4) inhibitors, which prevent the breakdown of endogenous GLP-1, or long-acting GLP-1 analogues such as exenatide maintain their efficacy in older patients and should be considered as appropriate therapeutic interventions in this age group.
It has been recognized for years that glucose can stimulate its own uptake in the absence of insulin. This is known as non–insulin-mediated glucose uptake (NIMGU). Under fasting conditions in normal individuals, approximately 70% of glucose uptake occurs via NIMGU, and during a meal, approximately 50% of glucose uptake occurs by non–insulin-mediated mechanisms. Because many obese patients with type 2 diabetes have profound insulin resistance, NIMGU becomes increasingly important for glucose metabolism in older patients with type 2 diabetes. Unfortunately, NIMGU is also impaired in older patients with diabetes, further compromising their glycemic control.16 In the future, this metabolic abnormality may prove to be an important therapeutic target in the elderly. Exercise, a reduction in free fatty acid levels, and the administration of GLP have been shown to enhance non–insulin-mediated glucose uptake in elderly patients with diabetes, and it is possible that future therapies for diabetes in this age group may be directed not only to increasing insulin secretion and reversing insulin resistance, but also to enhancing NIMGU.17
Molecular Biology
There is very little information regarding molecular biologic abnormalities in elderly persons with diabetes. To date, there is no evidence that mutations in the glucokinase gene, which controls the glucose sensor of the beta cell, is defective in these patients.18 In skeletal muscle, insulin binds to its receptor, resulting in activation of the insulin receptor tyrosine kinase. Although insulin receptor number and affinity are normal, some evidence suggests that insulin receptor tyrosine kinase activity may be defective in elderly patients, which may contribute to insulin resistance.19 Normal aging is characterized by progressive mitochondrial dysfunction, and it is possible that mitochondrial dysfunction contributes to impairments in both insulin sensitivity and insulin release in these patients.20 Further studies are clearly needed to determine the subcellular defects that impair glucose metabolism in elderly patients with diabetes.
Glucose Counter-Regulation
 A variety of studies have shown that the risk of severe or fatal hypoglycemia associated with the use of insulin or oral agents increases exponentially with age.21 There are several reasons for this phenomenon. The most important counter-regulatory hormone in the defense against hypoglycemia in normal subjects is glucagon, and the responses of this hormone to hypoglycemia are impaired in normal elderly subjects and, to an even greater extent, in elderly patients with diabetes22 (Figure 4). Many elderly patients have not been educated about the warning signs of hypoglycemia and, as a consequence, do not know how to interpret these symptoms when they occur.2 In addition, even when they are educated about them, elderly patients have reduced awareness of the autonomic warning symptoms of hypoglycemia. Finally, older patients have impaired psychomotor performance when their blood sugars are low, which prevents them from taking the appropriate steps to return their blood sugars to normal. Thus, the increased severity of hypoglycemia in the elderly is due to a variety of abnormalities, including decreased counter-regulatory hormone secretion, reduced knowledge and awareness of warning symptoms, and altered psychomotor performance.
A variety of studies have shown that the risk of severe or fatal hypoglycemia associated with the use of insulin or oral agents increases exponentially with age.21 There are several reasons for this phenomenon. The most important counter-regulatory hormone in the defense against hypoglycemia in normal subjects is glucagon, and the responses of this hormone to hypoglycemia are impaired in normal elderly subjects and, to an even greater extent, in elderly patients with diabetes22 (Figure 4). Many elderly patients have not been educated about the warning signs of hypoglycemia and, as a consequence, do not know how to interpret these symptoms when they occur.2 In addition, even when they are educated about them, elderly patients have reduced awareness of the autonomic warning symptoms of hypoglycemia. Finally, older patients have impaired psychomotor performance when their blood sugars are low, which prevents them from taking the appropriate steps to return their blood sugars to normal. Thus, the increased severity of hypoglycemia in the elderly is due to a variety of abnormalities, including decreased counter-regulatory hormone secretion, reduced knowledge and awareness of warning symptoms, and altered psychomotor performance.
Based on the above information, there are a number of interventions that could be expected to prevent hypoglycemia in the elderly. First, older patients should be educated carefully and frequently about the warning symptoms of hypoglycemia. Consideration should also be given to using oral agents or insulin, such as glipizide or insulin glargine, which have been associated with a lower frequency of hypoglycemia in elderly patients.
Conclusion
Diabetes in the elderly is caused by a combination of environmental and genetic factors that are superimposed on normal age-related changes in carbohydrate metabolism. Metabolic alterations in older people with diabetes are distinct from those that occur in the young. Because of these distinct metabolic abnormalities, the therapeutic approach to older patients should be different. Further understanding of the pathophysiology of diabetes in the elderly will allow us to better cope with the epidemic of this illness in the coming decades.
The author reports that he is a paid advisory board member for Merck and has received research grants from Merck in the past.
Dr. Meneilly is Professor and Head, Department of Medicine, The University of British Columbia, Vancouver, Canada.
References
1. Meneilly GS. Pathophysiology of diabetes in the elderly. In: Sinclair AJ, ed. Diabetes in Old Age. West Sussex, UK: Wiley-Blackwell; 2009:3-13.
2. Kahn CR. Banting Lecture. Insulin action, diabetogenes, and the cause of type II diabetes. Diabetes 1984;43:1066-1094.
3. Lipton RB, Liao Y, Cao G, et al. Determinants of incident non-insulin-dependent diabetes mellitus among blacks and whites in a national sample. The NHANES I epidemiologic Follow-up Study. Am J Epidemiol 1993;138: 826-839.
4. Muller DC, Elahi D, Tobin JD, Andres R. The effect of age on insulin resistance and secretion: A review. Semin Nephrol 1996;16:289-298.
5. Iozzo P, Beck-Nielsen J, Laakso M, et al. Independent influence of age on basal insulin secretion in non-diabetic humans. European Group for the Study of Insulin Resistance. J Clin Endocrinol Metab 1999;84:863-868.
6. Ferrannini E, Vichi S, Beck-Nielsen H, et al. Insulin action and age. European Group for the Study of Insulin Resistance. Diabetes 1996;45;947-953.
7. Meneilly GS, Tessier D. Diabetes in elderly adults. J Gerontol A Biol Sci Med Sci 2001;56:M5-M13.
8. Knowler WC, Barrett-Connor E, Fowler SE, et al; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention of metformin. N Engl J Med 2002;346:393-403.
9. Del Prato S. Role of glucotoxicity and lipotoxicity in the pathophysiology of Type 2 diabetes mellitus and emerging treatment strategies. Diabet Med 2009;26:1185-1192.
10. DeFronzo RA. Banting Lecture. From the triumvirate to the ominous octet: A new paradigm for the treatment of type 2 Diabetes mellitus. Diabetes 2009;58:773-795.
11. Arner P, Pollare T, Lithell H. Different aetiologies of type 2 (non-insulin dependent) diabetes mellitus in obese and non-obese subjects. Diabetologia 1991;34:483-487.
12. Meneilly GS, Elliott T, Tessier D, et al. NIDDM in the elderly. Diabetes Care 1996;19:1320-1375.
13. Meneilly GS, Elliott T. Metabolic alterations in middle-aged and elderly obese patients with type 2 diabetes. Diabetes Care 1999; 22:112-118.
14. Meneilly GS, Elahi D. Metabolic alterations in middle-aged and elderly lean patients with Type 2 diabetes. Diabetes Care 2005;28:1498-1499.
15. Naik RG, Brooks-Worrell BM, Palmer JP. Latent autoimmune diabetes in adults. J Clin Endocrinol Metab 2009;94:4635-4644. Published Online: October 16, 2009.
16. Forbes A, Elliott T, Tildesley H, et al. Alterations in non-insulin-mediated glucose uptake in the elderly patient with diabetes. Diabetes 1998;47:1915-1919.
17. Meneilly GS, McIntosh CH, Pederson RA, et al. Effect of glucagon-like peptide 1 on non-insulin-mediated glucose uptake in the elderly patient with diabetes. Diabetes Care 2001;24:1951-1956.
18. McCarthy MI, Hitman GA, Hitchins M, et al. Glucokinase gene polymorphisms; A genetic marker for glucose intolerance in cohort of elderly Finnish men. Diabet Med 1994;11:198-204.
19. Obermaier-Kusser B, White MF, Pongratz DE, et al. A defective intramolecular autoactivation cascade may cause the reduced kinase activity of the skeletal muscle insulin receptor from patients with non-insulin-dependent diabetes mellitus. J Biol Chem 1989;264:9497-9504.
20. Hawley JA, Lessard SJ. Mitochondrial function: Use it or lose it. Diabetologia 2007;50:699-702.
21. Stepka M, Rogala H, Czyzyk A. Hypoglycemia; A major problem in the management of diabetes in the elderly. Aging (Milano) 1993;5:117-121.
22. Meneilly GS, Cheung E, Tuokko H. Counterregulatory hormone responses to hypoglycemia in the elderly patient with diabetes. Diabetes 1994;43:403-410.
23. Thomson FJ, Masson EA, Leeming JT, Boulton AJ. Lack of knowledge of symptoms of hypoglycaemia by elderly diabetic patients. Age Aging 1991;20:404-406.