
A Man With a 15-Year History of Dermal Cysts on the Abdomen

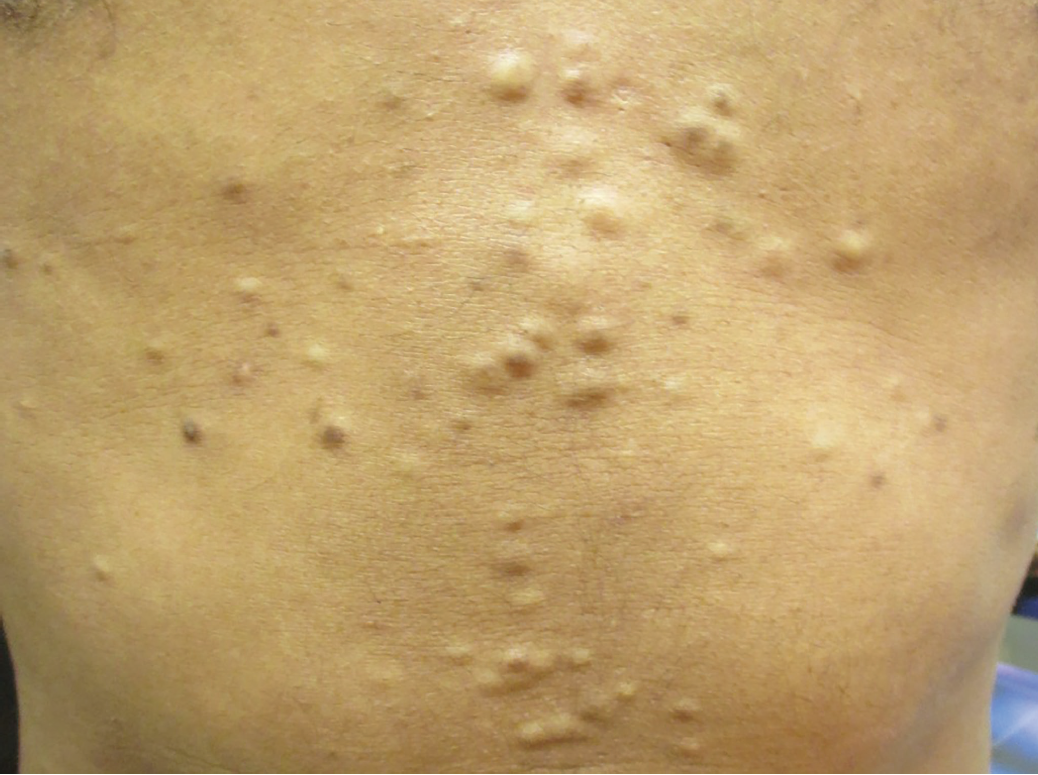
A 30-year-old man presented with a 15-year history of numerous, asymptomatic, skin-colored lesions on the abdomen. The lesions had increased in number and size very slowly since their initial appearance. His past medical history was noncontributory. No family members had similar lesions. He had been treated with oral isotretinoin without much success.
Physical examination revealed numerous, soft, skin-colored, cystic papules and nodules that were diffusely distributed on the abdomen and chest. The hair and nails appeared normal.
What’s Your Diagnosis?
A. Syringomas
B. Eruptive vellus hair cysts
C. Lipomatosis
D. Steatocystoma multiplex
See answer on next page.
Answer: Steatocystoma multiplex
is a hamartomatous malformation of the pilosebaceous unit characterized by multiple skin-colored, cystic papules and nodules that contain an oily substance comprised of sebum.1 The condition was first described by Jamieson in 1873, and the term steatocystoma multiplex was coined by Pringle in 1899.2
EPIDEMIOLOGY
The onset tends to occur during adolescence and early adulthood.1,3 Occasionally, the condition can appear earlier, only to worsen at puberty, when the activity of the sebaceous glands is high.3 Steatocystoma multiplex has been described at birth and in patients in their 50s.1,4 There is no sex predilection.5
ETIOPATHOGENESIS
Familial cases are often caused by mutations in the keratin 17 gene, KRT17, and have an autosomal dominant mode of inheritance.6 The gene has been mapped to chromosome 17 (band 17q21.2). The majority of cases are sporadic.5,7 Steatocystoma multiplex has been reported to be associated with pachyonychia congenita type 2 (Jackson-Lawler syndrome), hypertrophic lichen planus, acrokeratosis verruciformis, hypohidrosis, and eruptive vellus hair cysts.8
HISTOPATHOLOGY
Histologically, steatocystomas are mid-dermal cysts lined by an eosinophilic and wavy layer of thin, keratinized epithelium that lacks the granular layer.1 Sebaceous glands usually are present in the cyst wall.5 Cysts contain keratin, vellus hairs, and sebum.9
CLINICAL MANIFESTATIONS
Clinically, steatocystoma multiplex is characterized by multiple, asymptomatic, smooth, round, soft, movable, yellow to skin-colored papules and nodules.4,5 Lesions tend to be a few millimeters to a centimeter in diameter and are slow-growing. Superficial lesions usually are yellowish, while deeper lesions are skin-colored.5 The overlying epidermis is normal, with no central punctum present.5 The content is usually oily or creamy. Sites of predilection include the trunk (especially the presternal area), neck, axillae, proximal extremities, and groin, where high numbers of sebaceous glands are found.3,4 The face, scalp, and genital area also may be affected.10 There is usually little or no nail or hair involvement. There are no systemic manifestations.7
Several variants exist. In the suppurative variant, the lesions become inflamed and suppurative after minor trauma.7 In the acral variant, the lesions appear on the distal upper or lower extremities.1,4 The female to male ratio is 4 to 1.1 Localized forms of steatocystoma multiplex also have been described, such as cases with a cephalic or genital localization.11
DIAGNOSIS and Differential Diagosis
The diagnosis usually is clinical, based on typical physical findings. There are no abnormal laboratory findings. Skin biopsy or referral to a dermatologist can be helpful.
The differential diagnosis includes syringomas, lipomatosis, neurofibromatosis, leiomyomas, eruptive vellus hair cysts, milia, epidermal inclusion cysts, trichilemmal cysts, blue rubber bleb nevus syndrome, and Gardner syndrome. Inflamed steatocystoma multiplex may simulate hidradenitis suppurativa and acne conglobata.
COMPLICATIONS AND PROGNOSIS
Steatocystoma multiplex is cosmetically unsightly and may have an adverse impact on quality of life. The lesions can become infected and painful. Rarely, the lesions may calcify.5 Malignant degeneration has rarely been described.9
Without treatment, the lesions tend to persist and may slowly enlarge.
MANAGEMENT
Because the condition is benign and asymptomatic, treatment is not necessary except for cosmetic reasons. Treatment often is difficult, because the lesions are located deeply in the dermis, and their destruction is critical to prevent recurrence while minimizing the risk of scarring.3 Treatment options include needle aspiration, incision and drainage, surgical excision, intralesional corticosteroids, liquid nitrogen cryotherapy, and laser therapy.3
Alexander K. C. Leung, MD, is clinical professor of pediatrics at the University of Calgary and a pediatric consultant at the Alberta Children’s Hospital in Calgary, Alberta, Canada.
Benjamin Barankin, MD, is a dermatologist and the medical director and founder of the Toronto Dermatology Centre in Toronto, Ontario, Canada.
REFERENCES:
- Marzano AV, Tavecchio S, Balice Y, Polloni I, Veraldi S. Acral subcutaneous steatocystoma multiplex: a distinct subtype of the disease? Australas J Dermatol. 2012;53(3):198-201.
- Jamieson WA. Case of numerous cutaneous cysts scattered over the body. Edinb Med J. 1873;19(1):223-225.
- Bakkour W, Madan V. Carbon dioxide laser perforation and extirpation of steatocystoma multiplex. Dermatol Surg. 2014;40(6):658-662.
- Rollins T, Levin RM, Heymann WR. Acral steatocystoma multiplex. J Am Acad Dermatol. 2000;43(2):396-399.
- Rahman MH, Islam MS, Ansari NP. Atypical steatocystoma multiplex with calcification. ISRN Dermatol. 2011;2011:381901.
- Liu Q, Wu W, Lu J, Wang P, Qiao F. Steatocystoma multiplex is associated with the R94C mutation in the KRT17 gene. Mol Med Rep. 2015;12(4):5072-5076.
- Gordon Spratt EA, Kaplan J, Patel RR, Kamino H, Ramachandran SM. Steatocystoma. Dermatol Online J. 2013;19(12):20721.
- Ha W-W, Wang J, Wang W, et al. A novel missense mutation of keratin 17 gene in a Chinese family with steatocystoma multiplex. Ann Dermatol. 2013;25(4):508-510.
- Kromann CB, Zarchi K, Nürnberg BM, Jemec GBE. Recurring axillary, abdominal and genitofemoral nodules and abscesses: a quiz. Acta Derm Venereol. 2015;95(1):121-123.
- Jeong SY, Kim JH, Seo SH, Son SW, Kim IH. Giant steatocystoma multiplex limited to the scalp. Clin Exp Dermatol. 2009;34(7):e318-e319.
- Mortazavi H, Taheri A, Mansoori P, Kani ZA. Localized forms of steatocystoma multiplex: case report and review of the literature. Dermatol Online J. 2005;11(1):22.