
Innovations in Incontinence: Diagnosis and Treatment of Overactive Bladder
ABSTRACT: Overactive bladder (OAB) is an extremely common problem that affects women across the world and becomes more prevalent with age. In the last 15 to 20 years, numerous new medications and procedures have been introduced for the treatment of this syndrome. This article reviews the diagnosis of OAB and urge urinary incontinence and discusses the many available treatments.
KEYWORDS: Overactive bladder, urge urinary incontinence, antimuscarinic medication, β3-adrenergic receptor agonist, intradetrusor onabotulinumtoxinA, peripheral tibial nerve stimulation, sacral neuromodulation
Overactive bladder (OAB) is an extremely common problem that affects women across the world. OAB syndrome is defined as urinary urgency that usually is accompanied by frequency and nocturia, with or without urgency urinary incontinence, in the absence of urinary tract infection (UTI) or other obvious pathology.1 Studies have demonstrated that from 9% to 43% of women worldwide are affected by this condition,2 and that the prevalence and severity of symptoms increases with age. Women with obesity have a much higher risk of developing urge incontinence compared with women without obesity,3 and a dose-response relationship exists between body mass index (BMI) and the risk of urinary incontinence—that is, each 5-unit increase in BMI confers a 30% to 60% increased risk of developing incontinence over the next 5 years.3
OAB causes significant psychological and social distress and impacts the occupational, domestic, physical, and sexual domains of life.4,5 Depression, anxiety, work impairment, decreased sexual activity, and poorer health-related quality of life are all reported more commonly among women with incontinence.5 Women with severe OAB and urge incontinence often limit or avoid travel because of the fear of having an incontinence episode or not having an accessible toilet. Caregivers of elderly women with incontinence also are negatively impacted by the increased burden of managing incontinence.6 The costs of urinary incontinence also are substantial, rivaling those of conditions such as pneumonia, influenza, and arthritis.4

Classification and Causes
There are 3 main types of urinary incontinence: stress urinary incontinence, urge urinary incontinence, and mixed urinary incontinence (Table 1). Stress incontinence is the loss of urine with coughing, laughing, sneezing, or physical exertion. Urge incontinence is the loss of urine with urgency, which has been described as the sudden, compelling desire to pass urine that is difficult to defer.1 Women with mixed incontinence have both stress and urge incontinence. As indicated by this definition, OAB syndrome encompasses urge incontinence. The term OAB-dry sometimes is used to refer to women with urgency-frequency without urge incontinence, and OAB-wet refers to women with urge incontinence associated with wetting accidents.
The precise cause of OAB is not known, but the condition is thought to result from inappropriate contractions of the detrusor muscle. In the majority of women with it, the syndrome is idiopathic; however, a number of neurologic conditions are associated with OAB (eg, multiple sclerosis, stroke, Parkinson disease), and the formal definition is neurogenic detrusor overactivity.
 Evaluation of Incontinence
Evaluation of Incontinence
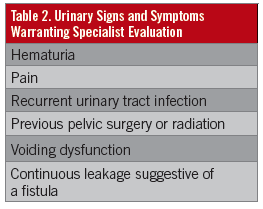
The first step in evaluating women with incontinence is taking a history and doing a physical examination. Providers should routinely ask women about urinary symptoms, including bothersome urgency, frequency, and incontinence episodes, since women may be embarrassed by their symptoms and therefore not readily divulge these concerns. The interview should focus on the timing, frequency, severity, duration, and the level of bother caused by urinary urgency, frequency, and incontinence. There is no cutoff for a normal number of voids per day; urinary frequency that is bothersome is considered abnormal. The incontinence type usually can be ascertained from a thorough history. Additionally, the provider should identify patients with symptoms warranting further evaluation by a specialist (Table 2).7
Because patients’ recollection of their voiding frequency often is inaccurate, a voiding diary can be a helpful adjunct to better characterize urinary frequency, incontinent episodes, and fluid intake. Numerous traditional paper diaries are available; additionally, apps are available for smartphones.
The physical examination of patients with incontinence should include gynecologic and neurologic evaluation. Pelvic exam focuses on assessment of vulvovaginal atrophy or genitourinary syndrome of menopause, palpation of the urethra to rule out urethral diverticulum or Skene duct cysts, evaluation for vaginal discharge (which many patients mistake for urine loss), and bimanual examination to evaluate for other gynecologic pathology including uterine fibroids and adnexal masses. A cough stress is a simple way to diagnose stress incontinence—observation of loss of urine during cough or Valsalva maneuver confirms this diagnosis. Measurement of urethral mobility with the use of the Q-tip test is no longer routinely performed.
Neurologic examination should include assessment of lower extremity strength, reflexes, and sensation, as well as assessment of perineal sensation/reflexes and pelvic floor muscle strength (Kegel exercises).
Postvoid residual urine volume also should be assessed to rule out overflow incontinence and can be checked with a 10-French in-out catheter or with a bladder scan. Residual volumes of less than 150 mL within 10 minutes of voiding generally are considered acceptable. Urinalysis with or without urine culture should be performed on all women with incontinence to rule out signs of UTI or microscopic hematuria. Urodynamic testing may help guide treatment in women with mixed incontinence. It helps characterize the type of incontinence when the diagnosis is unclear or when the patient has been refractory to empiric behavioral and medical management. Complex urodynamic testing or cystometry also are indicated in patients whose urethral function may be compromised, such as women with a history of pelvic radiation or previous gynecologic or lower urinary tract surgery, and women who do not respond to the initial therapy for urinary incontinence. Women with refractory incontinence should have cystoscopy to rule out underlying pathology of the lower urinary tract. Cystourethroscopy also is indicated for assessment of microscopic hematuria or elevated residual volumes.
OAB Treatment
Numerous innovations have occurred in the treatment of OAB in the last 15 to 20 years. Because this disorder is thought to result from inappropriate detrusor contractions, treatments target the prevention of detrusor muscle contraction. The American Urological Association (AUA) has published guidelines to assist clinicians in making evidence-based treatment decisions.2 Clinicians should explain to patients the pathophysiology of OAB and discuss goals of treatment. It is particularly important for patients to realize that most OAB treatments can significantly improve but not cure their symptoms, and that trial of several modalities, often in combination, may be necessary.
First-Line Treatments
The first-line treatment for OAB is behavioral therapy, which includes behavior modification, bladder training, and pelvic floor physical therapy. Studies have shown that behavioral therapies generally are as effective as pharmacologic therapy. A key component of behavioral modification is fluid restriction; many patients with bothersome urgency and frequency symptoms have an excessive fluid intake. Reduction to a total fluid intake of 48 to 64 oz is generally recommended, barring any medical indication for a higher intake. Elimination of potential “bladder irritants” such as caffeine, alcohol, and artificial sweeteners also may be beneficial.
Bladder training involves scheduled voiding: Over several weeks, patients progressively increase the time between voids, with the goal of achieving an interval of 2 to 4 hours between voids. Studies have shown more than a 50% reduction in incontinence episodes with timed voiding.8 Pelvic floor physical therapy helps patients identify and strengthen their levator ani muscles. Contraction of these muscles with the sensation of urinary urgency helps defer the sensation and allows additional time to reach a toilet.

Second-Line Treatments
Pharmacotherapy is the second-line treatment for OAB (Table 3). The guideline from the AUA and the Society of Urodynamics, Female Pelvic Medicine, and Urogenital Reconstruction (SUFU)2 indicates that medications may be started concurrently with behavioral therapy, or in cases where behavioral therapy alone has been inadequate. The 2 classes of medications approved for treatment of OAB are muscarinic receptor antagonists/anticholinergics and β3-adrenergic receptor agonists.
Antimuscarinic medications. These agents target M3 muscarinic receptors in the bladder with varying levels of specificity. Parasympathetic activation of these receptors results in detrusor contraction. Numerous antimuscarinic medications have been approved in the United States for the treatment of OAB, and no consistent evidence suggests the superiority of one antimuscarinic agent over another.7,9
A recent systematic review and meta-analysis found a reduction in voids of 2.06 per day with antimuscarinics and of 1.2 per day with placebo, and a reduction in incontinence episodes of 1.73 per day with antimuscarinics and of 1.06 per day with placebo.9 Patients should be aware that a trial of 4 to 8 weeks is necessary to determine efficacy of antimuscarinic therapy. If inadequate response is achieved, the dose may be titrated to a higher amount, or another agent may be tried. Most health insurances cover 1 or 2 anticholinergic medications, and it is reasonable to try the least expensive medication first.
The typical adverse effects of antimuscarinics include dry mouth, dry eyes, constipation, and cognitive impairment. While these effects are not life threatening, they can be quite bothersome and result in high discontinuation rates and poor compliance rates. By 12 months after initiation of antimuscarinics, approximately 65% to 78% of patients discontinue therapy,10,11 and by 2 years as many as 86% discontinue therapy.11 In general, extended-release formulations should be prescribed preferentially to immediate release formulations, since they have fewer adverse effects. Of note, oxybutynin is available over the counter as a transdermal patch and confers the lowest risk of anticholinergic adverse effects. Antimuscarinics should not be used in patients with narrow-angle glaucoma, impaired gastric emptying, or a history of urinary retention.2
β3-adrenergic receptor agonists. The newest medication available for the treatment of OAB is mirabegron, a β3-adrenergic receptor agonist. A meta-analysis of the medication’s phase 3 clinical trials showed that mirabegron, 50 mg, reduced incontinence episodes by 1.49 versus 1.09 with placebo, and voids per day were reduced by 1.75 with mirabegron versus 1.20 with placebo.12 In its analysis of therapy with mirabegron, 5 antimuscarinic agents, and placebo, the United Kingdom’s National Institute for Health and Care Excellence found that mirabegron was similar to the antimuscarinic agents in reduction of frequency, urgency, and urinary incontinence, with the exception of solifenacin, which was statistically more effective, although this difference was small. Mirabegron is generally very well tolerated and does not cause the dry eyes, dry mouth, and constipation typical of antimuscarinic agents. A dose-related increase in heart rate and blood pressure occurs, although the average increases are less than 2 beats/min and less than 1 mm Hg.2 While the cardiovascular effects of mirabegron are minimal, it is prudent to avoid its use in women with severe uncontrolled hypertension.

Third-Line Treatments
Third-line treatments are available for women who do not achieve adequate improvement in their symptoms with behavioral therapy and pharmacotherapy, or for women who cannot tolerate medications due to adverse effects. Three treatments have been approved by the U.S. Food and Drug Administration (FDA) for refractory OAB: intradetrusor onabotulinumtoxinA, peripheral tibial nerve stimulation (PTNS), and sacral nerve stimulation (SNS, also called sacral neuromodulation).
Intradetrusor onabotulinumtoxinA. OnabotulinumtoxinA is a potent neurotoxin that inhibits the presynaptic release of acetylcholine at the neuromuscular junction. Injection into the detrusor muscle effectively reduces its ability to contract. A Cochrane Database meta-analysis of randomized, placebo-controlled trials of onabotulinumtoxinA for OAB found that it reduced urinary frequency by 3.37 episodes per day and reduced incontinence episodes by 2.74 per day at 12 weeks after treatment.13
OnabotulinumtoxinA consistently has been found to increase both bladder capacity and voided urine volume. The Pelvic Floor Disorders Network performed a randomized, double-blind, double-placebo-controlled trial comparing onabotulinumtoxinA, 100 U, and solifenacin, 5 mg or 10 mg.14 The treatment groups had similar reductions in urge incontinence episodes (solifenacin 3.4 vs onabotulinumtoxinA 3.3, P = .81) and quality of life measures, but significantly more women in the onabotulinumtoxinA group achieved complete continence than in the solifenacin group (27% vs 13%, P = .003). A recent systematic review and meta-analysis of 8 randomized, controlled trials enrolling 1320 patients found mean reductions of 1.68 incontinence episodes/day and 1.82 voids/day, with 4.89 higher odds of achieving complete continence with onabotulinumtoxinA treatment.15
Intradetrusor injection of 100 U of onabotulinumtoxinA is FDA-approved for treatment of idiopathic OAB, and 200 U is approved for neurogenic OAB. The injections are performed cystoscopically, typically in the clinic or outpatient setting with administration of intravesical local anesthetic. The onabotulinumtoxinA is distributed across the posterior wall of the bladder in multiple injections—typically 20 injections for the 100 U dose and 30 injections for the 200 U dose (Figure 1). The procedure is generally very well tolerated, but some patients may require intravenous sedation in the operating room.
The most common adverse effects of intradetrusor onabotulinumtoxinA injection are urinary retention and UTI. From 5% to 8% of patients treated with the 100-U dose will require intermittent self-catheterization to manage elevated postvoid residual.15,16 Up to 19% of patients develop UTI, and periprocedural antibiotic prophylaxis is indicated to mitigate this risk.15
Peripheral tibial nerve stimulation. PTNS is a neuromodulation therapy that involves afferent stimulation of the posterior tibial nerve. The posterior tibial nerve arises from spinal levels L4 through S3, which overlap with the parasympathetic inputs to the bladder from S2 through S4. Chinese acupuncturists have known for hundreds of years that stimulation of the area 4 to 5 cm superior to the medial malleolus, which is the site of stimulation for PTNS, improves urinary incontinence symptoms (Figure 2).
The typical treatment regimen for PTNS is a 12-week course of once-weekly 30-minute treatment sessions, followed by maintenance therapy as needed (often about once per month). Several randomized, controlled trials of PTNS have demonstrated that 54.5% to 79.5% of patients have improvement in their OAB symptoms compared with 0 to 20.9% of control subjects treated with placebo and 54.8% of control subjects treated with the antimuscarinic agent tolterodine.16-18 Compared with sham treatments, a 12-week course of PTNS resulted in significant reductions of 2.4 to 4.1 voids/day, 0.7 episodes of nocturia, and 1.3 to 2.3 incontinence episodes/day.17,19 Randomization to PTNS or tolterodine revealed a similar reduction in voids per day, nocturia, and incontinence episodes per day with both treatments, but significantly more patients in the PTNS group reported marked or moderate improvement in their symptoms (79.5% vs 54.8% P = .0118). Three-year follow-up data from 50 patients who responded to an initial 12-week PTNS course and continued maintenance therapy showed that 97% continued to report marked or moderate improvement in their symptoms, and that they maintained an average reduction of 2.7 voids/day, 0.7 episodes of nocturia, and 2.0 episodes of incontinence per day.
PTNS is generally very well tolerated; the main adverse effect is minor irritation at the stimulation site. Patients with pacemakers require clearance from their cardiologist before initiating therapy. Patients typically find the noninvasiveness of PTNS attractive, but the required weekly sessions for the initial treatment course may be unappealing, especially for patients who are working or do not drive. PTNS is not currently available for or approved for home use in the United States.
Sacral nerve stimulation. SNS is another neuromodulation technique that is FDA-approved for the treatment of refractory OAB. As with PTNS, the exact mechanism of SNS is unknown, but it is thought to modulate the afferent and efferent signals to the bladder.
SNS is the most invasive of the 3 treatment options for refractory OAB; it involves implantation of leads directly into the sacral foramina to directly stimulate the S3 nerve roots, as well as implantation of a subcutaneous pacemaker-like stimulator (Figure 3). The procedure involves a test phase followed by permanent implantation. The test phase placement of leads into the S3 foramina may be performed either with percutaneous placement of wires or with subcutaneous tunneling of the permanent leads. In order to move on to the permanent implantation of the stimulator, patients must complete a 2-week voiding diary and demonstrate greater than 50% improvement in their urgency, frequency, or incontinence episodes. The permanent stimulator usually is placed under the skin of the upper buttock.
The reported success rates in the literature for stage 1 range from approximately 50% to 80%.2,20 Most studies of SNS are single-arm trials and have found significant improvement in voiding parameters and quality of life measures.2 One prospective multicenter study followed the cases of 152 women with severe OAB for 5 years after they underwent the SNS procedure. At 5 years after surgery, 68% of women with OAB-wet and 56% of women with OAB-dry reported a greater than 50% improvement in symptoms. The mean number of leakage episodes per day decreased from 9.6 at baseline to 4.9 at 1-year follow-up, and decreased further to 3.9 at 5-year follow-up. The mean number of voids per day decreased from 19.3 at baseline to 13.0 at 1-year follow-up, and increased slightly to 13.8 at 5-year follow-up.21
Adverse events occur much more commonly with SNS than with PTNS; 3.3% to 19.8% of patients report pain at the stimulator site, 2.2% to 14.3% report infection or irritation at the site, and 6.3% to 39.5% report the need for surgical revision.2
The AUA-SUFU guideline advises that “SNS is an appropriate therapy that can have durable treatment effects but in the context of frequent and moderately severe adverse events, including the need for additional surgeries.”2
It is rare that a woman with OAB does not have adequate improvement with any of the treatments discussed here, either alone or in combination. For women with symptoms of this level of severity, extreme surgical treatments such as augmentation cystoplasty or urinary diversion may be considered.
The variety of therapies now available for the treatment of OAB allows practitioners many more options to customize treatment for the individual patient. Primary care providers should feel comfortable with diagnosis of the different types of incontinence and are encouraged to initiate first- and second-line treatments for OAB. Referral to a urogynecologist or urologist is warranted for certain concerning urinary symptoms discussed above, as well as for patients with refractory OAB for a discussion of more-advanced treatment options.
REFERENCES:
- Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010; 29(1):4-20.
- Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. https://www.auanet.org/common/pdf/education/clinical-guidance/Overactive-Bladder.pdf. Published May 2014. Accessed November 3, 2015.
- Subak LL, Richter HE, Hunskaar S. Obesity and urinary incontinence: epidemiology and clinical research update. J Urol. 2009;182(6 suppl):S2-S7.
- Tubaro A. Defining overactive bladder: epidemiology and burden of disease. Urology. 2004;64(6 suppl 1):2-6.
- Coyne KS, Sexton CC, Irwin DE, Kopp ZS, Kelleher CJ, Milsom I. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int. 2008;101(11):1388-1395.
- Gotoh M, Matsukawa Y, Yoshikawa Y, Funahashi Y, Kato M, Hattori R. Impact of urinary incontinence on the psychological burden of family caregivers. Neurourol Urodyn. 2009;28(6):492-496.
- Lucas MG, Bosch RJL, Burkhard FC, et al. EAU guidelines on assessment and nonsurgical management of urinary incontinence. Eur Urol. 2012;62(6):1130-1142.
- Fantl JA, Wyman JF, McClish DK, et al. Efficacy of bladder training in older women with urinary incontinence. JAMA. 1991;265(5):609-613.
- Reynolds WS, McPheeters M, Blume J, et al. Comparative effectiveness of anticholinergic therapy for overactive bladder in women: a systematic review and meta-analysis. Obstet Gynecol. 2015;125(6):1423-1432.
- Yeaw J, Benner JS, Walt JG, Sian S, Smith DB. Comparing adherence and persistence across 6 chronic medication classes. J Manag Care Pharm. 2009;15(9):728-740.
- Chancellor MB, Migliaccio-Walle K, Bramley TJ, Chaudhari SL, Corbell C, Globe D. Long-term patterns of use and treatment failure with anticholinergic agents for overactive bladder. Clin Ther. 2013;35(11):1744-1751.
- Nitti VW, Khullar V, van Kerrebroeck P, et al. Mirabegron for the treatment of overactive bladder: a prespecified pooled efficacy analysis and pooled safety analysis of three randomised, double-blind, placebo-controlled, phase III studies. Int J Clin Pract. 2013;67(7):619-632.
- Duthie JB, Vincent M, Herbison GP, Wilson DI, Wilson D. Botulinum toxin injections for adults with overactive bladder syndrome. Cochrane Database Syst Rev. 2011;(12):CD005493.
- Visco AG, Brubaker L, Richter HE, et al; Pelvic Floor Disorders Network. Anticholinergic therapy vs. onabotulinumtoxinA for urgency urinary incontinence. N Engl J Med. 2012;367(19):1803-1813.
- Cui Y, Zhou X, Zong H, Yan H, Zhang Y. The efficacy and safety of onabotulinumtoxinA in treating idiopathic OAB: a systematic review and meta-analysis. Neurourol Urodyn. 2015;34(5):413-419.
- Nitti VW, Dmochowski R, Herschorn S, et al; EMBARK Study Group. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase 3, randomized, placebo controlled trial. J Urol. 2013;189(6):2186-2193.
- Peters KM, Carrico DJ, Perez-Marrero RA, et al. Randomized trial of percutaneous tibial nerve stimulation versus sham efficacy in the treatment of overactive bladder syndrome: results from the SUmiT trial. J Urol. 2010;183(4):1438-1443.
- Peters KM, MacDiarmid SA, Wooldridge LS, et al. Randomized trial of percutaneous tibial nerve stimulation versus extended-release tolterodine: results from the Overactive Bladder Innovative Therapy trial. J Urol. 2009;182(3):1055-1061.
- Finazzi-Agrò E, Petta F, Sciobica F, Pasqualetti P, Musco S, Bove P. Percutaneous tibial nerve stimulation effects on detrusor overactivity incontinence are not due to a placebo effect: a randomized, double-blind, placebo controlled trial. J Urol. 2010;184(5):2001-2006.
- Siddiqui NY, Wu JM, Amundsen CL. Efficacy and adverse events of sacral nerve stimulation for overactive bladder: a systematic review. Neurourol Urodyn. 2010;29(suppl 1):S18-S23.
- van Kerrebroeck PEV, van Voskuilen AC, Heesakkers JPFA, et al. Results of sacral neuromodulation therapy for urinary voiding dysfunction: outcomes of a prospective, worldwide clinical study. J Urol. 2007;178(5):2029-2034.