
Helping Adolescents Kick the Habit
A PARENT ASKS:
I have just found out that my 17-year-old daughter is smoking cigarettes. How am I going to get her to quit?
THE PARENT COACH ADVISES:
Providing parents with effective guidance to help their child quit smoking is of the utmost importance for primary care pediatricians and family medicine physicians. Tobacco use in adolescence is a public health problem that needs to be addressed on the national, community, school, and individual level.1 Tobacco use is the leading cause of preventable death in the United States,2 and it is responsible for a large portion of annual U.S. health care expenditures.2
 The majority of cigarette smoking–associated mortality presents in the adult population; nevertheless, the roots of tobacco addiction are planted during adolescence and young adulthood. Nearly 90% of adult tobacco users smoked their first cigarette before the age of 18 years; 10% of current adolescent users smoked their first whole cigarette before the age of 13 years.2,3 In 2011, 23% of high school students reported using tobacco, and 18% reported current cigarette use (defined as having smoked a cigarette on at least 1 day during the 30 days prior to having taken the survey), falling short of the U.S. Department of Health and Human Services’ “Healthy People 2020” goal of 16%.3 These striking statistics highlight the great need for pediatric health care providers to be skilled in smoking cessation.
The majority of cigarette smoking–associated mortality presents in the adult population; nevertheless, the roots of tobacco addiction are planted during adolescence and young adulthood. Nearly 90% of adult tobacco users smoked their first cigarette before the age of 18 years; 10% of current adolescent users smoked their first whole cigarette before the age of 13 years.2,3 In 2011, 23% of high school students reported using tobacco, and 18% reported current cigarette use (defined as having smoked a cigarette on at least 1 day during the 30 days prior to having taken the survey), falling short of the U.S. Department of Health and Human Services’ “Healthy People 2020” goal of 16%.3 These striking statistics highlight the great need for pediatric health care providers to be skilled in smoking cessation.
Why do adolescents start smoking? The decision to smoke is influenced by many personal, social, and environmental factors.2 Parental smoking is the leading predictor of adolescent smoking. Other risk factors for teen smoking include easy access to cigarettes, low levels of parental monitoring, a lack of restrictions on smoking in the home, and a perceived high prevalence of smoking among peers. Moreover, patients with mental health disorders such as mood disorders or anxiety have a higher incidence of smoking.4
While evidence-based guidelines exist for adult tobacco cessation, evidence about adolescent tobacco cessation is sparse. Clinical trials are plagued by small sample sizes and high rates of attrition.2,5 In addition, patterns of adolescent smoking vary more than those of adults. Most adult smokers are daily smokers with nicotine dependence, whereas only an estimated 20% of adolescent smokers have a physiologic dependence on tobacco products.6 One recent publication describes the stages of smoking as follows: (1) not smoking; (2) preparing to smoke, considering smoking; (3) initiating smoking; (4) irregular smoking or nondaily use; and (5) regular, daily smoking.2 Because there are various stages of smoking, the definition of smoking used in studies also varies, which makes it difficult to compare study findings. Furthermore, a teenager may not self-identify as a smoker but may have tried one cigarette or may smoke irregularly.
Child advocacy groups have recognized the need for pediatric smoking cessation guidelines. The American Academy of Pediatrics (AAP), for example, has published numerous articles in the past several years about adolescent tobacco use.4,7,8
Addressing tobacco with teenagers. Among the most important parts of the cessation process is the establishment of a respectful physician–patient relationship. The AAP recommends approaching this process by using the 6 A’s: anticipate, ask, advise, assess, assist, and arrange follow-up (Table 1).6 Pediatric clinicians should include tobacco education in anticipatory guidance, discuss the health effects of tobacco, and be aware of the populations at increased risk of tobacco initiation. They should ask about tobacco use, identifying and documenting the tobacco use status and exposure to secondhand smoke of every patient at every visit, as well as advise every tobacco user to quit. The clinician should assess the patient’s willingness to attempt cessation—ie, the patient’s stage of change—by asking questions such as the following:
• Does the patient have no interest in quitting? (precontemplative stage)
• Is he or she thinking about quitting? (contemplative stage)
• Has he or she set a quit date? (preparation stage)
• Has he or she already quit? (action stage)
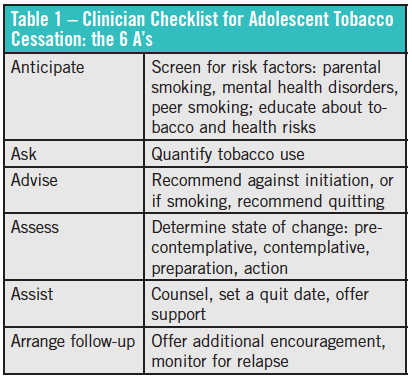
Next, pediatric clinicians should assist with the cessation attempt by providing brief counseling, setting a quit date, and making a referral to community, school, or online programs for additional counseling and support; then arrange follow-up to provide additional encouragement and prevent relapse.6
The steps to becoming tobacco-free. After a patient’s readiness to quit has been assessed, it is time to assist in quitting. If the patient is in the precontemplative stage of change, providing brief counseling and encouraging quitting in a nonjudgmental manner leaves the door open for future support. If the child’s parents also smoke, offer them similar counseling. Recommend a smoke-free environment at home and in the car, without exceptions.7 The AAP advises that all clinicians be familiar with pharmaceutical options for smoking cessation and offer them to parents if needed.7 Ensure close follow-up with parents and adolescents to reassess stages of change at each visit.
For the patient who is willing to attempt cessation, brief counseling can be done in the office. Suggest that the adolescent schedule a quit date that he or she shares with parents, friends, and siblings.6 Prior to that quit date, the patient should prepare by planning ways to avoid situations that may trigger smoking and identifying coping mechanisms.
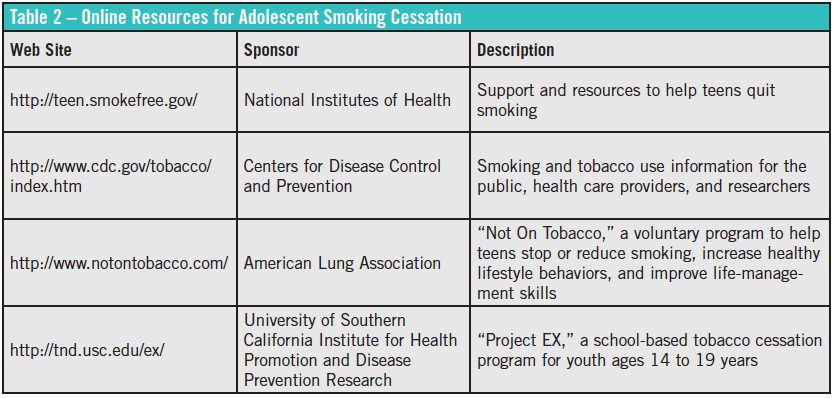
The AAP encourages health care providers to become familiar with and active in local community- and school-based smoking cessation programs and to refer patients to these programs.7 While research on the effectiveness of these programs is limited, two national programs have been found to be effective9: the American Lung Association’s “Not On Tobacco” program, and “Project EX,” developed at the University of Southern California. In addition, the National Institutes of Health (NIH) national quit line, 1-800-QUIT-NOW, can provide telephone-based counseling sessions specific to teenage smoking.7 The Centers for Disease Control and Prevention and the NIH also offer teen-focused education and tobacco cessation Web sites (Table 2).1
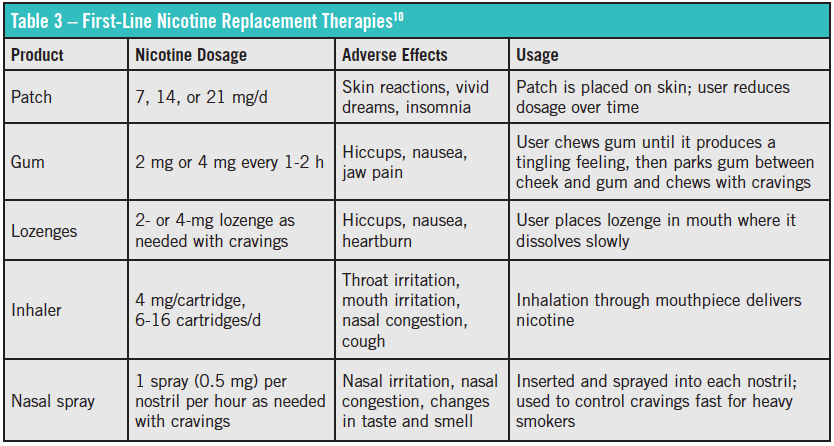
What about medication? The AAP has not recommended pharmacotherapy for adolescents under the age of 18 years. Although nicotine replacement therapy is thought to be safe in adolescents, limited evidence supports its use in this population (Table 3).2,7,10 The antidepressant bupropion has failed to show benefit in patients younger than 18, despite its efficacy in adult patients.2,5 Varenicline, a nicotinic receptor partial agonist, has not been well-studied in the adolescent population and is not recommended in patients under 18 years of age.2,5,7
After a smoking cessation plan has been put into effect, the clinician should schedule a folow-up visit within the first week after the patient’s quit date tol monitor progress. Future visits with the patient and family should include monitoring for relapse. As with adults, quitting may take numerous tries, but the more quit attempts an adolescent makes, the more likely his or her cessation is to be permanent.
References:
1. US Department of Health and Human Services. Preventing Tobacco Use Among Youth and Young Adults: A Report of the Surgeon General. Atlanta, GA: US Dept of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2012. http://www.surgeongeneral.gov/library/
reports/preventing-youth-tobacco-use/full-report.pdf. Accessed July 5, 2013.
2. Patnode CD, O’Connor E, Whitlock EP, Perdue LA, Soh C. Primary Care Relevant Interventions for Tobacco Use Prevention and Cessation in Children and Adolescents: A Systematic Evidence Review for the U.S. Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality; 2012. Evidence Synthesis 97. AHRQ publication 12-05175-EF-1. http://www.ncbi.nlm.nih.gov/books/NBK114973/pdf/TOC.pdf. Accessed July 5, 2013.
3. Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance — United States, 2011. MMWR Surveill Summ. 2012;61(4):1-162. http://www.cdc.gov/mmwr/pdf/ss/ss6104.pdf. Accessed July 5, 2013.
4. Sims TH; Committee on Substance Abuse. Technical report—tobacco as a substance of abuse. Pediatrics. 2009;124(5):e1045-e1053. http://pediatrics.aappublications.org/content/124/5/e1045.full.pdf. Accessed July 5, 2013.
5. Grimshaw G, Stanton A. Tobacco cessation interventions for young people. Cochrane Database Syst Rev. 2006;(4):CD003289. doi:10.1002/14651858.CD003289.pub4.
6. Adelman WP. Tobacco use cessation for adolescents. Adolesc Med Clin. 2006;17(3):697-717.
7. Committee on Environmental Health, Committee on Substance Abuse, Committee on Adolescence, Committee on Native American Child Health. Policy statement—tobacco use: a pediatric disease. Pediatrics. 2009;124(5):1474-1487. http://pediatrics.aappublications.org/content/124/5/1474.full.pdf. Accessed July 5, 2013.
8. Committee on Substance Abuse. Tobacco’s toll: implications for the pediatrician. Pediatrics. 2001;107(4):794-798. http://pediatrics.aappublications.org/content/107/4/794.full.pdf. Accessed July 5, 2013.
9. Breland A, Colby S, Dino G, Smith G, Taylor M. Youth Smoking Cessation Interventions: Treatments, Barriers and Recommendations for Virginia. Richmond: Virginia Commonwealth University Institute for Drug and Alcohol Studies; 2009. http://www.vcu.edu/idas/vytp/reports/index.html. Accessed July 5, 2013.
10. Medication guide. National Institutes of Health, smokefree.gov. http://www.smokefree.gov/medication-guide.aspx. Accessed July 5, 2013.