
Ebola Virus Disease: An Update on Diagnosis, Treatment, and Prevention
ABSTRACT: Since 1976, several outbreaks of Ebola virus disease (EVD) have occurred. With a prolonged incubation period and variable clinical presentations, EVD is a challenge to manage. Diagnostic and therapeutic advances following the most recent outbreak have improved prognosis. Several experimental preventive measures, including vaccination, also are available. Health care providers must be aware of EVD’s long-term sequelae in patients, and ongoing monitoring necessary. When a patient presents with a possible case of EVD, immediate prevention and infection control measures must be undertaken. Knowledge of available resources and notifying the appropriate federal health agencies is key to successful management of this potentially devastating disease.
KEYWORDS: Ebola, public health, infection control
Ebola virus was first identified in 1976 when an outbreak of Ebola hemorrhagic fever occurred in Zaire (now the Democratic Republic of the Congo). A second outbreak occurred later that year in Sudan. The virus, which is thought to have originated in fruit bats, was first detected near the Ebola River in Zaire. These 2 outbreaks had approximately 300 victims each, but the disease’s effects were limited by the regions’ remoteness. The Zaire outbreak was the first time the disease had been recognized, and it had an 88% mortality rate.1 The Sudan virus was less virulent but still dangerous, with a 53% mortality rate.1
During the Zaire outbreak, Dr. Ngoy Mushola recorded the first clinical description of the Ebola virus disease (EVD) in his clinical log: “The illness is characterized with a high temperature of about 39°C, hematemesis, diarrhea with blood, retrosternal abdominal pain, prostration with ‘heavy’ articulations, and rapid-evolution death after a mean of three days.”2
Most Ebola virus outbreaks have originated in sub-Saharan Africa and have traveled only to other countries via the shipment of nonhuman primates, via travel of infected persons, or through accidental contamination in testing facilities. The Reston Ebola virus was identified in the United States in 1989 when macaque monkeys imported from the Philippines to Reston, Virginia, were found to have a virus similar to the identified Ebola species. More than 150 animal handlers were tested for Ebola; only 6 were found to have developed antibodies to it, and none developed Ebola hemorrhagic fever. The Centers for Disease Control and Prevention (CDC) concluded that this Reston Ebola virus has a low infection rate in humans.
Ivory Coast Ebola virus was discovered in 1994 when a scientist conducting autopsies on chimpanzees in the Tai Forest contracted Ebola hemorrhagic fever. This strain was found to be different from the Zaire or Sudan strains, and the case has been the only report of Ivory Coast Ebola occurring in humans.
Approximately 18 major outbreaks of Ebola virus have occurred in Africa since 1976. The most recent outbreak started in March 2014 in Guinea in West Africa and rapidly spread to neighboring Sierra Leone and Liberia. The outbreak was traced to a 1-year-old child who died in December 2013. On August 8, 2014, the World Health Organization (WHO) declared the epidemic to be an international public health emergency. It was the largest Ebola outbreak ever documented and the first recorded in this area of West Africa.
As of November 12, 2015, the WHO had reported 28,599 suspected cases and 11,299 Ebola deaths in Guinea, Liberia, and Sierra Leone—figures that may be underestimated.3 Health care workers have been especially vulnerable to this outbreak and represent an estimated 10% of deaths. Two imported cases, including 1 death, and 2 locally acquired cases in health care workers have been reported in the United States.1 As of October 15, 2014, a total of 17 cases of Ebola had been treated outside of Africa, 4 of which were fatal.
In a September 2014, statement, the WHO said, “The Ebola epidemic ravaging parts of West Africa is the most severe acute public health emergency seen in modern times. Never before in recorded history has a biosafety level four pathogen infected so many people so quickly, over such a broad geographical area, for so long.”4 The current outbreak has been improving rapidly because of engaged and effective governmental leadership, coordination between local and international authorities, and strong engagement of local communities. On August 5, 2015, the WHO reported 2 confirmed cases of Ebola in the week ending August 2—one in Guinea and one in Sierra Leone.3 This was the lowest weekly total since March 2014 and marked the third consecutive decline in weekly case incidence, perhaps signaling that the epidemic is close to an end.
From August 2014 to November 2014, an unrelated outbreak of Ebola affected 66 persons, causing 47 deaths, in the Democratic Republic of the Congo.1
Clinical Presentation
The incubation period for EVD is from 2 to 21 days. In one study,5 presentation to a hospital was 3 to 7 days after the onset of symptoms. Initial symptoms are sudden-onset fever greater than 38.3°C, along with nonspecific symptoms such as fatigue, malaise, myalgia, arthralgia, headache, and sore throat. Nausea, vomiting, abdominal pain, diarrhea, conjunctivitis, and rash may follow. Cutaneous flushing or a nonpruritic, maculopapular, centripetal rash are common. Later, hemorrhagic symptoms such as epistaxis, hematuria, hematemesis, and melena may occur. Due to the uncharacteristic clinical presentation early in the disease, it can be difficult to distinguish EVD from other diseases such as malaria, typhoid fever, hepatitis, meningitis, and dengue. The presentation of abrupt illness, a high fever of less than 3 weeks’ duration, and at least 2 hemorrhagic symptoms without any predisposing factors should be enough to begin supportive treatment until laboratory confirmation is available.6
The vascular bed is the main target of Ebola virus, and disseminated intravascular coagulation may become the dominant clinical feature. Seizures and coma also can occur. Patients whose symptoms do not improve by the end of the first week usually die from multiorgan failure and hypovolemic shock. Analysis of cases during the 2014 outbreak revealed that most patients died 7 to 11 days after symptom onset.5 Older age is associated with worse outcomes. In previous outbreaks, the mortality rate ranged from 30% to 90%. Patients who are able to mount an immune response begin to recover in approximately 7 to 10 days and experience a period of slow, prolonged convalescence.
Diagnosis
EVD has a variable clinical presentation and thus epidemiologic data must be taken into consideration. EVD usually is transmitted through direct mucous membrane or percutaneous exposure to infected body fluids such as blood, stool, and vomit, so specific questions about contact with sick or dead persons is important during history-taking.7 Any illness with onset of fever and no response to treatment for the usual causes of fever in the area, along with at least 1 of the following signs: bloody diarrhea, bleeding from gums, bleeding into skin (purpura), and bleeding into the eyes and urine, meets the WHO definition for a suspected Ebola case. Specimen collection, transport, and laboratory testing should follow biosafety recommendations. The patient’s blood sample typically is sent abroad to a biosafety level 4 laboratory for diagnostic confirmation.
For early detection of EVD in suspected or probable cases, viral RNA by reverse-transcription polymerase chain reaction (RT-PCR) testing or viral antigen by enzyme-linked immunosorbent assay (ELISA) are the recommended methods.8 A serious potential exists for false-positive and false-negative results with sole reliance on a single method; thus, RT-PCR with antigen-capture ELISA is more useful.9 A second specimen should be collected if the first was collected less than 3 days after the onset of symptoms and tested negative. Ebola virus RNA is detected very early after infection, before the antigen or antibody test results are positive. Viral antigen is detectable in the blood 3 to 6 days after symptom onset and could disappear 7 to 16 days after symptom onset or antigen load in the blood is correlated with symptoms.
ELISA tests for IgM and IgG antibodies are specific. IgM antibodies to Ebola virus appear between 2 and 9 days after symptoms begin and disappear between and 30 and 168 days. IgG antibodies appear between 6 and 18 days after symptom onset and persist for months. The absence of specific reagents for antibody tests, such as Ebola antigens and polyclonal anti-Ebola antibodies, make such tests generally unavailable where they are most needed.
Other laboratory findings include leukopenia followed by leukocytosis and atypical lymphocytosis; thrombocytopenia; elevation of aminotransferase levels; prolongation of partial thromboplastin time and international normalized ratio; and electrolyte abnormalities.
Immunohistochemistry testing of formalin-fixed postmortem skin specimens is an alternative diagnostic method used to study the role of contact transmission in Ebola hemorrhagic fever.10
Treatment
No U.S. Food and Drug Administration (FDA)-approved vaccines or therapeutics are available for prevention, postexposure prophylaxis, or treatment of EVD; therefore, the initial focus is on preventing spread. The use of personal protective equipment, the proper recognition and monitoring of exposures, proper burial habits, and isolation protocols can help decrease disease spread.11
Patients with EVD should receive care in designated treatment centers and by clinicians trained to care for such patients.12 Since treating these patients requires a multidisciplinary approach,13 community care centers have been established in parts of West Africa to isolate patients awaiting Ebola diagnostic test results and to provide basic care to patients with confirmed EVD pending transfer to Ebola treatment units.14 Survivors can be discharged once they no longer have signs and symptoms of EVD and have 2 negative PCR tests on whole blood, separated by at least 48 hours.8
Supportive Care
Supportive care includes volume repletion, maintenance of blood pressure, maintenance of oxygenation, pain control, nutritional support, and treatment of secondary bacterial infections and preexisting comorbidities.15
Patients in the early phase of illness who respond to oral antiemetic and antidiarrheal therapy may take in sufficient fluids by mouth to prevent or correct dehydration,7 but later stages require intravenous fluids to replace lost volume. Other supportive measures include antipyretic agents to decrease fever and analgesic agents to manage pain. Dose reduction of these agents may be needed for patients with progressive hepatic dysfunction. Nonsteroidal anti-inflammatory drugs generally are avoided to help minimize the risk of renal failure, which can contribute to mortality in EVD.
Blood products (ie, packed red blood cells, platelets, fresh frozen plasma) also are given to patients with coagulopathy and bleeding. Total parenteral nutrition also has benefited patients with poor oral intake.16 Renal replacement therapy also may be required to manage severe multifactorial acute kidney injury.17 Empiric antimicrobial treatment also should be administered to patients with clinical evidence of bacterial sepsis, with adequate coverage for gram-negative pathogens.18 Respiratory support including ventilators also may be needed.
Repurposed Antiviral Agents
Brincidofovir (CMX001) is an acyclic nucleotide analogue being developed for the treatment of poxvirus, cytomegalovirus, and other DNA virus infections. The drug has been evaluated in patients in phase 2 and 3 trials but has not been approved for licensure.19
Favipiravir (T-705, Avigan) is a nucleoside analogue that inhibits the replication of a wide range of RNA viruses.20 This agent has been approved in Japan for the treatment of influenza and is undergoing phase 3 trials for influenza in the United States and other countries.
Ebola-Specific Medications
ZMapp has been used on an emergency basis to treat a physician and a nurse successfully in the United States.21 ZMapp is a combination of 3 monoclonal antibodies that bind to the virus so that the body can clear it.22
TKM-Ebola is a preparation of small interfering RNA that targets 3 different Ebola virus genes.23 A phase 1 trial of TKM-Ebola that began in January 2014 was put on hold because of fever in some subjects; however, the FDA has modified its action to allow the drug to be administered under compassionate-use protocols.
The nucleoside analogue BCX4430 inhibits viral RNA polymerase function, acting as a nonobligate RNA chain terminator, and is being produced for potential administration to humans.24
Nucleic acid analogues known as phosphorodiamidate morpholino oligomers are being developed for the treatment of a number of medical conditions including filovirus infections.25
Vaccines
The vesicular stomatitis virus (VSV) vaccine has protected macaques when administered shortly after virus challenge.26 During the 2014-2015 outbreak in West Africa, it was administered as postexposure prophylaxis to 2 health care workers who had sustained a percutaneous injury with a needle that had come in contact with a contaminated glove.27 Follow-up testing using RT-PCR testing found no evidence of EVD.
The University of Sierra Leone College of Medicine and Allied Health Sciences, the Sierra Leone Ministry of Health and Sanitation, and the CDC are working together on a candidate Ebola vaccine trial in Sierra Leone, which launched in April 2015. This study, called the Sierra Leone Trial to Introduce a Vaccine against Ebola (STRIVE), is designed to assess the safety and efficacy of rVSV-ZEBOV.
Convalescent Plasma
Convalescent plasma comes from the blood of survivors to utilize their antibodies to help clear the virus.22 Whole blood from convalescent patients was used to treat 8 individuals with Ebola virus disease near the end of the 1995 outbreak in Kikwit, the Democratic Republic of the Congo.28
Long-Term Sequelae
A study of survivors from the 2007 Ebola epidemic showed several long-term sequelae, including higher-risk of retro-orbital pain, blurred vision, hearing loss, difficulty swallowing, difficulty sleeping, arthralgia, and other constitutional symptoms. Chronic health problems, memory loss, and confusion also were reported.29 Psychosocial issues, including survivor guilt, financial difficulties, difficulty reintegrating, and consequences of stigma associated with Ebola, also are a concern for survivors.30,31 A study is ongoing in Liberia measuring the effects of Ebola on patients 2 years after infection.32
Ebola virus has been isolated from semen of convalescent patients.33 In response, the WHO has published advice about reducing the risk of sexual transmission from convalescing patients.34 Ebola virus has been found in the aqueous humor in a patient 9 weeks after clearance of viremia, and it was associated with a change of eye color from blue to green. This patient also developed severe, unilateral uveitis.35
Public Health Precautions
Staff members at outpatient clinics, physician’s offices, public health clinics, and hospital centers should be on the alert for individuals who might have EVD (Table 1).36 A patient with a febrile illness might have an infectious etiology other than Ebola, but one should ask whether during the previous 21 days the individual has traveled to a country known to be having an Ebola outbreak. If so, these measures must be taken immediately: Isolate the patient; avoid unnecessary contact with individual; wear personal protection equipment (PPE); inform the health department; and organize transfer to a specific facility able to evaluate, diagnose, and, if needed, treat the patient. Under no circumstances is the patient to be transported to another facility unless public health authorities have been notified.
No one in the ambulatory care setting should have direct contact with a person under investigation for Ebola without wearing PPE.37,38 If PPE is available, and direct patient contact is necessary, a single staff member (trained in proper donning and removal of PPE) should be designated to interact with the patient. At a minimum, health care workers should use the following PPE before direct patient contact: a face shield and surgical facemask, an impermeable gown, and 2 pairs of gloves. Depending on the circumstances (eg, the patient is bleeding, vomiting, or having copious diarrhea), full gear needs to be used.38 The designated staff member should refrain from direct interaction with other staff and patients in the office until PPE has been safely removed in a designated, confined area. Examples of safe donning and removal of PPE should be reviewed. Transport should be informed about the individual’s potential EVD, and precaution for emergency medical services personnel should be initiated at the point of arriving at the outpatient facility.
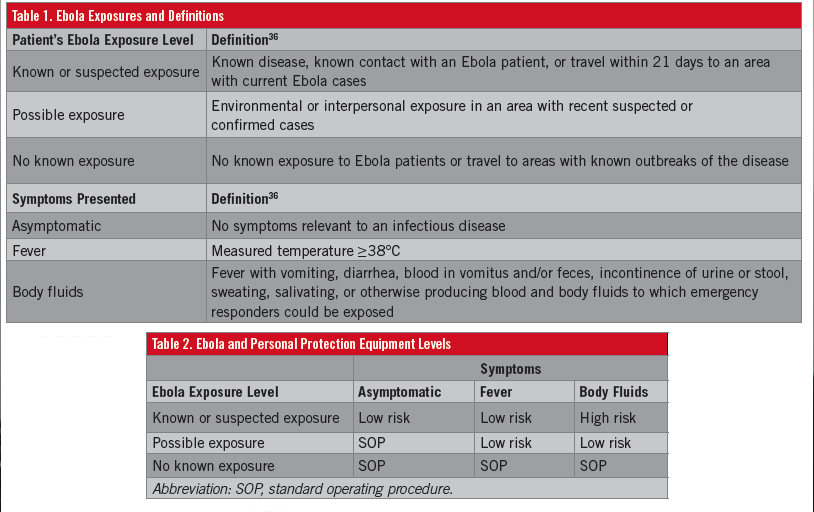
Three possible PPE levels are recommended, depending on circumstances (Table 2):
• Standard operating procedure (SOP)-recommended PPE, which corresponds to the PPE dictated by the standard operating procedure (SOP) of the organization as dictated by CDC guidance and the state or local jurisdiction.
• Low-risk PPE, an increased protection level corresponding to an increased likelihood of responder or health care worker exposure.
• High-risk PPE, the highest recommended protection level corresponding to a high likelihood of responder exposure.
Coordination of public health systems is in place to monitor individuals with potential EVD. Usually this process starts with airport screening (eg, travel from affected areas or having contact with someone with confirmed Ebola virus, fever, headache, muscle pain, weakness, fatigue, diarrhea, vomiting, abdominal pain, or hemorrhage). The patient will be actively monitored for at least 21 days following travel. These patients are referred to an Ebola assessment hospital. Not every hospital is equipped to receive an EVD patient; only some are able to isolate and care for a patient until a definitive diagnosis is confirmed or ruled out.
Once the patient is at the Ebola assessment hospital, 2 different situations may arise. The first one is an individual who has fever and mild symptoms. In such a case, initial isolation and evaluation can be done following airborne precautions. The second one is an individual with more severe symptoms such as fever, vomiting, diarrhea, or obvious bleeding. In this scenario, full isolation and PPE must be used.
Because of the lag in time between clinical suspicions of EVD, the isolation of the patient, and laboratory testing, the Ebola assessment hospital must have enough equipment available to isolate the patient. PPE for staff for at least 4 to 5 days is necessary to ensure safe patient care. The hospital staff members must be trained in the proper use of PPE, including proper donning, removal, and waste management.
Once the patient has been confirmed as having EVD, proper treatment is indicated at an Ebola treatment center for the total duration of the patient’s illness. The CDC’s Ebola Response Team (CERT) is ready to be deployed to any Ebola treatment center to provide assistance and is available 24 hours a day, 7 days a week, for consultation with hospitals and state and local health departments by calling the CDC Emergency Operation Center at (770) 488-1700 or by e-mail at eocreport@cdc.gov.
Laboratory Evaluation
Ebola testing should be performed on an individual meeting strict criteria including fever, headache, nausea, vomiting, diarrhea, abdominal pain, obvious bleeding, and an epidemiologic risk exposure within the previous 21 days. If the patient is deemed to be a person under investigation, at least 4 mL of whole blood for an adult and 1 mL for a pediatric patient should be obtained in a plastic collection tube with EDTA. The blood sample should be kept cold at 2°C to 8°C with cold packs to 1 of the at least 50 designated LRN (Laboratory Response Network) laboratories in the United States. If the patient has had symptoms for less than 3 days, a second sample may be necessary to rule out Ebola. The receiving laboratory should be informed about the blood sample so that safety precautions can be made at the receiving facility to mitigate possible exposure of laboratory personnel to Ebola.
The blood sample should be packaged with a triple packaging system: a primary container (a sealable specimen container) wrapped with absorbent material; a second container (watertight and leak-proof); and an outer shipping package.
Diagnostic testing is performed with RT-PCR for Ebola virus at any LRN laboratory. These laboratories use an FDA-approved emergency-use-only assay for the Ebola (Zaire species) virus. Samples that test positive are considered presumptively positive for Ebola Zaire RNA by RT-PCR are then submitted to the CDC for additional evaluation.
Prevention
No FDA-approved vaccines are available for EVD; however, some experimental vaccines are available in affected areas. When traveling to an endemic area of Ebola virus, the following precautions are suggested:
• Practice careful hygiene (wash with soap and water or alcohol-based hand sanitizer).
• Avoid contact with body fluids.
• Avoid funerals or burial rituals that require washing the body of a person who has died of EVD.
• Avoid contact with bats and nonhuman primates, or blood, fluids, or raw meat prepared from these animals.
• Avoid contact with semen from men who have had Ebola until the virus is no longer detected in the semen.
• After returning from an endemic area, watch for signs and symptoms of Ebola for at least 21 days.
For health care workers who have the potential to be exposed to an individual with Ebola, the following steps must be followed:
• Wear appropriate PPE.
• Follow proper infection control and sterilization procedures.
• Isolate patients with Ebola from other patients.
• Avoid direct unprotected contact with the bodies of people who have died from Ebola.
• Notify health officials if you have been in contact with blood or body fluids of a person with Ebola virus.
Environmental Infection Control in Hospitals
Results of limited laboratory studies under favorable conditions indicate that Ebola virus can remain viable in solid surfaces for a prolonged period of time.39 No epidemiologic evidence suggests that Ebola virus is transmitted via the environment or fomites (eg, bedrails, door knobs, laundry). However, hospitals are recommended to take the following steps40:
• Environmental services staff wears PPE to protect against direct skin and mucous membrane exposure to cleaning chemicals, contamination, and splashes or spatters during environmental cleaning and disinfection.
• Use a hospital disinfectant registered with the U.S. Environmental Protection Agency to disinfect environmental surfaces in the room of patients under investigation for or with confirmed Ebola.
• Avoid contamination of reusable porous surfaces that cannot be made single-use.
• Routinely clean and disinfect the PPE doffing area.
• Discard all linens and non–fluid-impermeable curtains into the waste stream and dispose of appropriately.
Because Ebola virus is a category A infectious substance regulated by the U.S. Department of Transportation’s hazardous material regulations (HMR), the substance must be packaged and transported in accordance with the HMR. n
For more, please visit our
Infectious Disease Medical
Resource Center at ww.consultant360.com.
References:
- Centers for Disease Control and Prevention. Outbreaks chronology: Ebola virus disease. http://www.cdc.gov/vhf/ebola/outbreaks/
- history/chronology.html. Updated November 10, 2015. Accessed November 12, 2015.
- Bardi JS. Death called a river. Scripps Research Institute News and Views. 2002;2(1). https://www.scripps.edu/newsandviews/e_20020114/ebola1.html. Accessed November 12, 2015.
- World Health Organization. Ebola data and statistics. http://apps.who.int/gho/data/view.ebola-sitrep.ebola-summary-20150807?lang=en. Accessed November 12, 2015.
- World Health Organization. Experimental therapies: growing interest in the use of whole blood or plasma from recovered Ebola patents (convalescent therapies). http://www.who.int/mediacentre/news/ebola/26-september-2014/en/. Published September 26, 2014. Accessed August 9, 2014.
- Bah EI, Lamah M-C, Fletcher T, et al. Clinical presentation of patients with Ebola virus disease in Conakry, Guinea. N Engl J Med. 2014;372(1):40-47.
- Borio L, Inglesby T, Peters CJ, et al. Hemorrhagic fever viruses as biological weapons: medical and public health management. JAMA. 2002;287(18):2391-2405.
- Chertow DS, Kleine C, Edwards JK, Scaini R, Giuliani R, Sprecher A. Ebola virus disease in West Africa—clinical manifestations and management. N Engl J Med. 2014;371(22):2054-2057.
- World Health Organization. Laboratory diagnosis of Ebola virus disease. http://apps.who.int/iris/bitstream/10665/134009/1/WHO_EVD_GUIDANCE_LAB_14.1_eng.pdf. September 19, 2014. Accessed November 12, 2015.
- Towner JS, Rollin PE, Bausch DG, et al. Rapid diagnosis of Ebola hemorrhagic fever by reverse transcription-PCR in an outbreak setting and assessment of patient viral load as a predictor of outcome. J Virol. 2004;78(8):4330-4341.
- Zaki SR, Shieh W-J, Greer PW, et al. A novel immunohistochemical assay for the detection of Ebola virus in skin: implications for diagnosis, spread, and surveillance of Ebola hemorrhagic fever. J Infect Dis. 1999;179(suppl 1):S36-S47.
- Breman JG, Johnson KM. Ebola then and now. N Engl J Med. 2014;371(18):1663-1666.
- Centers for Disease Control and Prevention. Interim guidance for U.S. hospital preparedness for patients under investigation (PUIs) or with confirmed Ebola virus disease (EVD): a framework for a tiered approach. http://www.cdc.gov/vhf/ebola/healthcare-us/preparing/hospitals.html. Updated August 28, 2015. Accessed November 12, 2015.
- Decker BK, Sevransky JE, Barrett K, Davey RT, Chertow DS. Preparing for critical care services to patients with Ebola. Ann Intern Med. 2014;161(11):831-832.
- Logan G, Vora NM, Nyensuah TG, et al. Establishment of a community care center for isolation and management of Ebola patients — Bomi County, Liberia, October 2014. MMWR Morb Mortal Wkly Rep. 2014;63(44):1010-1012.
- Centers for Disease Control and Prevention. Ebola virus disease (EVD) information for clinicians in U.S. healthcare settings. http://www.cdc.gov/vhf/ebola/healthcare-us/preparing/clinicians.html. Updated November 9, 2015. Accessed November 12, 2015.
- Johnson DW, Sullivan JN, Piquette CA, et al. Lessons learned: critical care management of patients with Ebola in the United States. Crit Care Med. 2015;43(6):1157-1164.
- Connor MJ Jr, Kraft C, Mehta AK, et al. Successful delivery of RRT in Ebola virus disease. J Am Soc Nephrol. 2015;26(1):31-37.
- Kreuels B, Wichmann D, Emmerich P, et al. A case of severe Ebola virus infection complicated by gram-negative septicemia. N Engl J Med. 2014;371(25):2394-2401.
- Chimerix announces emergency investigational new drug applications for brincidofovir authorized by FDA for patients with Ebola virus disease [news release]. Durham, NC: Chimerix; October 6, 2014. http://ir.chimerix.com/releasedetail.cfm?releaseid=874647. Accessed November 12, 2015.
- Furuta Y, Gowen BB, Takahashi K, Shiraki K, Smee DF, Barnard DL. Favipiravir (T-705), a novel viral RNA polymerase inhibitor. Antiviral Res. 2013;100(2):446-454.
- Lyon GM, Mehta AK, Varkey JB, et al; Emory Serious Communicable Diseases Unit. Clinical care of two patients with Ebola virus disease in the United States. N Engl J Med. 2014;371(25):2402-2409.
- Nebraska Medicine. Ebola outbreak: the Nebraska Ebola method. http://www.nebraskamed.com/biocontainment-unit/ebola. Accessed November 12, 2015.
- Arbutus Biopharma. TKM-Ebola & TKM-Ebola-Guinea. http://arbutusbio.com/portfolio/tkm-ebola.php. Accessed November 12, 2015.
- Biocryst Pharmaceuticals Inc. BCX4430. http://www.biocryst.com/bcx_4430. Accessed November 12, 2015.
- Warren TK, Shurtleff AC, Bavari S. Advanced morpholino oligomers: a novel approach to antiviral therapy. Antiviral Res. 2012;94(1):80-88.
- Feldmann H, Jones SM, Daddario-DiCaprio KM, et al. Effective post-exposure treatment of Ebola infection. PLoS Pathog. 2007;3(1):e2.
- Lai L, Davey R, Beck A, et al. Emergency postexposure vaccination with vesicular stomatitis virus-vectored Ebola vaccine after needlestick. JAMA. 2015;313(12):1249-1255.
- Mupapa K, Massamba M, Kibadi K, et al; International Scientific and Technical Committee. Treatment of Ebola hemorrhagic fever with blood transfusions from convalescent patients. J Infect Dis. 1999;179(suppl 1):S18-S23.
- Clark DV, Kibuuka H, Millard M, et al. Long-term sequelae after Ebola virus disease in Bundibugyo, Uganda: a retrospective cohort study. Lancet Infect Dis. 2015;15(8):905-912.
- Lee-Kwan SH, DeLuca N, Adams M, et al. Support services for survivors of Ebola virus disease — Sierra Leone, 2014. MMWR Morb Mortal Wkly Rep. 2014;63(50):1205-1206.
- De Roo A, Ado B, Rose B, Guimard Y, Fonck K, Colebunders R. Survey among survivors of the 1995 Ebola epidemic in Kikwit, Democratic Republic of Congo: their feelings and experiences. Trop Med Int Health. 1998;3(11):883-885.
- Study of Ebola survivors opens in Liberia [news release]. Bethesda, MD: National Institutes of Health; June 17, 2015. http://www.nih.gov/news-events/news-releases/study-ebola-survivors-opens-liberia. Accessed November 12, 2015.
- Rowe AK, Bertolli J, Khan AS, et al; Commission de Lutte contre les Epidémies à Kikwit. Clinical, virologic, and immunologic follow-up of convalescent Ebola hemorrhagic fever patients and their household contacts, Kikwit, Democratic Republic of the Congo. J Infect Dis. 1999;179(suppl 1):S28-S35.
- World Health Organization. Interim advice on the sexual transmission of the Ebola virus disease. http://www.who.int/reproductivehealth/topics/rtis/ebola-virus-semen/en/. Published May 8, 2015. Accessed November 12, 2015.
- Varkey JB, Shantha JG, Crozier I, et al. Persistence of Ebola virus in ocular fluid during convalescence. N Engl J Med. 2015;372(25):2423-2427.
- Centers for Disease Control and Prevention. Ebola (Ebola virus disease). http://www.cdc.gov/vhf/ebola/healthcare-us/evaluating-patients/case-definition.html. Updated January 26, 2015. Accessed November 12, 2015.
- Centers for Disease Control and Prevention Healthcare Infection Control Practices Advisory Committee (HICPAC). Figure: example of safe donning and removal of personal protective equipment (PPE). http://www.cdc.gov/hicpac/2007IP/2007ip_fig.html. Updated December 29, 2009. Accessed November 12, 2015.
- Centers for Disease Control and Prevention. Guidance on personal protective equipment (PPE) to be used by healthcare workers during management of patients with confirmed Ebola or persons under investigation (PUIs) for Ebola who are clinically unstable or have bleeding, vomiting, or diarrhea in U.S. hospitals, including procedures for donning and doffing PPE. http://www.cdc.gov/vhf/ebola/healthcare-us/ppe/guidance.html. Updated August 27, 2015. Accessed on November 12, 2015.
- Sagripanti JL, Lytle DC. Sensitivity to ultraviolet radiation of Lassa, vaccinia, and Ebola viruses dried on surfaces. Arch Virol. 2011;156(3):489-494.
- Centers for Disease Control and Prevention. Interim guidance for environmental infection control in hospitals for Ebola virus. http://cdc.gov/vhf/ebola/healthcare-us/cleaning/hospitals.html. Updated April 27, 2015. Accessed November 12, 2015.