
Dissecting Thoracic Aortic Aneurysm With Left-Sided Hemothorax
Aortic aneurysm is defined as a swelling or bulging to more than 1.5 times the normal size in any section of the aorta.1 Aortic aneurysms may occur anywhere along the course of the aorta, from the abdomen to the thorax. Patients with ruptured aneurysms can have a variety of symptoms on presentation, depending on the location of the aneurysm and the area where the bleeding occurs. Dissecting thoracic aortic aneurysms are usually catastrophic events with acute symptoms, including severe chest pain; however, in older people, the pain can be mild. We present the case of a dissecting thoracic aortic aneurysm in a 76-year-old man whose symptoms were atypical, resulting in a delayed diagnosis partly because his condition stabilized with nonspecific management. The discussion reviews the anatomy and physiology of the aorta; risk factors for developing an aortic aneurysm; and general management principles, including findings that should raise the clinical suspicion for this disorder, particularly in elders.
Case Report
A 76-year-old man with a medical history of angina, hypertension, and hypercholesterolemia visited the emergency department (ED) because of left-sided chest pain. On arrival, his vital signs were as follows: blood pressure (BP), 126/72 mm Hg; pulse, 103 beats per minute (BPM); and oxygen saturation, 98% on room air. The clinical examination was essentially normal, except that reduced air entry at the left base of the chest was noted on auscultation. While in the ED, the patient’s skin became pale, diaphoretic, and clammy, and his BP decreased to 102/70 mm Hg. His pulse remained stable at 101 BPM, but the oxygen saturation remained at 98% despite the administration of 15 L of oxygen via a nonrebreather mask. The initial laboratory results were as follows: white blood cell count, 19.1/µL (normal, 4500-11,000/µL); hemoglobin, 13.4 g/dL (normal, 12.5-16.0 g/dL); creatinine, 1.4 mg/dL (normal, 0.6-1.1 mg/dL), and 12-hour troponin I, 0.2 ng/L (normal, <0.04 ng/L).
An electrocardiograph revealed sinus tachycardia but no acute changes. His chest radiograph showed left basal consolidation with a small pleural effusion (Figure 1). The initial impression was that he had experienced a non–ST-segment elevation myocardial infarction (MI) and had sepsis related to a lower respiratory tract infection. His BP improved with intravenous (IV) fluids, and he was treated with IV co-amoxiclav and clarithromycin. The patient also received aspirin, clopidogrel, and enoxaparin for his suspected MI. His condition stabilized, but on day 2, his hemoglobin level fell to 9.4 g/dL and the antiplatelet agents and enoxaparin were stopped. Two units of whole blood were transfused and his hemoglobin level remained stable.

Over the next 10 days, there was an overall improvement despite ongoing antibiotic therapy for rising inflammatory markers and increasing dullness to percussion and decreased breath sounds on auscultation at the left lung. Repeated chest radiographs revealed a significantly worsened left-sided pleural effusion (Figure 2). After 2 weeks, the patient began to have episodes of pyrexia; therefore, a pleural aspiration was performed, revealing heavily blood-stained fluid. The culture of the pleural fluid was negative. At this point, an aortic dissection was suspected and a computed tomography (CT) scan of the thorax was done. The CT scan confirmed a 7-cm type B aortic dissection, which started distal to the subclavian artery (Figure 3).
A surgical opinion suggested conservative management, and the effusion was drained. He remained without overall improvement and received a further course of antibiotics for his suspected chest infection, until he improved clinically 2 weeks after his dissection was diagnosed. At the 4- and 10-month follow-up visits, the patient remained well and no long-term sequelae from the aneurysm were noted. The chest radiograph taken at 4-month follow-up revealed only left basal pleural thickening (Figure 4).

Discussion
Our case differs from normal presentations of dissecting aneurysms. Although the patient had acute symptoms on presentation, his conditioned stabilized with nonspecific management; therefore, the aortic dissection went undetected for 14 days. It is possible that the aortic dissection occurred on day 2 when his hemoglobin level decreased, with a small leak into the pleura causing the effusion that was seen on the chest radiograph. He may also have had a larger leak on day 14, which could have increased the pleural effusion.
The risk factors for atherosclerosis in this man’s case included smoking, hypertension, and hypercholesterolemia. Atherosclerosis and hypertension have been shown to increase the risk of developing aortic aneurysms and dissection. The review of the anatomy and histology of the aorta, characteristics of aortic aneurysms and dissections, and the consequences of aortic rupture that follows will help to place our case report in context.
Anatomy and Histology of the Aorta
The aorta is divided into the ascending aorta, the aortic arch, and the descending aorta. The ascending aorta, contained within the pericardium, starts at the upper left ventricle at the level of the third costal cartilage. It ascends obliquely for 5 cm and ends at the second right costal cartilage 6 cm posterior to the sternum. It has two branches, the right and left coronary arteries. The aortic arch curves backward and left, over the root of the left lung, ending at the fourth thoracic vertebra, where it branches again into the innominate, the left common carotid, and the left subclavian arteries. The descending aorta begins to the left of the vertebral column and approaches the midline, ending directly in front of the twelfth thoracic vertebra.
The aorta is an elastic artery consisting of tunica intima, tunica media, and tunica adventitia. The tunica intima is a single layer of flattened endothelial cells that regulate blood clotting and vascular tone. It also secretes nitric oxide and prostacyclin, which cause vasodilation and inhibit platelet aggregation, and endothelin-1, which causes vasoconstriction.2 The tunica media is broad, with concentric, fenestrated sheets of elastin, collagenous tissue, and few smooth muscle fibers. Elastic tissue allows expansion during systole and recoil during diastole. The collagenous tissue of the tunica adventitia contains the vasa vasorum of the aorta, which provides the artery with its blood supply.
Characteristics of Aortic Aneurysms
Aortic aneurysm is defined as a permanent, localized dilatation of the aorta, with a diameter at least 1.5 times the expected width.1,3 The incidence of thoracic aortic aneurysms is 5.9 to 10.4 per 100,000 persons annually.4,5 Some studies have shown a prevalence of 0.13% to 0.67%.5,6 Aortic aneurysms involve the ascending aorta in 51% of patients, the aortic arch in 11%, and the descending aorta in 38%.4 Thoracic aortic aneurysms grow at approximately 0.1 cm per year, and rapid growth is usually a result of intercurrent aortic dissection.7 Aortic aneurysms occur primarily from degeneration of the artery, most commonly in elderly patients with hypertension.3,8
Hypertension and atherosclerosis lead to fibrosis of the tunica intima, with degradation and apoptosis of smooth muscle cells in the tunica media.9 Elastic components in the artery stiffen and weaken, predisposing to aneurysm formation and rupture. Elastin in the arterial walls of the aneurysm is greatly reduced.8 The tunica media shows decreased smooth muscle cells and fragmentation of elastic fibers, which are related to cystic medial degeneration.8 This characteristic is found in some inherited collagen disorders, such as Ehlers-Danlos syndrome, and in Marfan syndrome, where the aneurysm is largest and often confined to the aortic root.3,10
Some research has implicated matrix metalloproteinase (MMP) enzymes found in the aortic wall as the prime agents of the deleterious changes seen in aortic disease.7 Marked elevations of MMP enzymes were found in patients in these studies, which was thought to cause increased enzymatic
destruction of fibrillin and collagen in the aortic wall.
Characteristics of Aortic Dissection
The incidence of aortic dissection is 0.5 to 3.0 per 100,000 persons per year.4,11 Prevalence is difficult to establish because many cases are not identified until the postmortem examination. Some studies have found a prevalence of between 0.1% and 38%.12,13 Dissections involve the ascending aorta in two-thirds of cases.14 Chronic arterial hypertension causing high shear stress inside the aorta is the most common acquired cause of aortic dissection.9 The initial tear may occur anywhere in the thoracic aorta, and hemorrhage through the tunica intima causes a false lumen in the tunica media.15
Dissection can occur independently from an aneurysm. Tamori and colleagues16 found that, of 140 patients with acute aortic dissection, 24% had coexisting aortic aneurysms. A clinical analysis of 3000 patients found that the critical diameters at which aortic aneurysms are more likely to dissect or rupture are 6 cm for the ascending aorta and 7 cm for the descending aorta.7 A mechanical analysis correlated with the clinical findings, showing that aneurysms larger than 6 cm have less capacity to stretch; thus, cardiac contraction force results in higher wall tension and stress. Aortic dissections are classified by two systems, Stanford17 and DeBakey.18
In the Stanford classification, dissections are placed into two categories: type A and type B. In type A, dissections occur in either the ascending aorta only or in both the ascending and descending aortas.17 In type B, dissections occur in the descending aorta only.17 The DeBakey classification assigns types of dissections as follows: in type I, the dissection occurs in both the ascending and descending aorta; in type II, it occurs in the ascending aorta; and in type III, it occurs in the descending aorta.18 Using these classification systems, our patient had the less common type B (Stanford) or type III (DeBakey) dissection. Although the DeBakey system is more specific, this article uses the Stanford system, as it relates better to the patient’s clinical management, which would be mainly surgical for type A and medical for type B.
Patients with aortic dissection typically have chest pain on presentation with or without syncope. As illustrated by our case, descending aortic dissections are likely to cause hemothorax because of the proximity of the descending thoracic aorta to the lungs. Both right- and left-sided hemorrhagic effusions can occur, but effusions on the left side are more common because of the anatomical relationship of the aorta to the left thoracic cavity. On the other hand, ascending dissections more commonly cause cardiac tamponade as they rupture into the pericardial sac or hemomediastinum.
Consequences of Aortic Rupture
Because the ascending aorta is contained within the pericardium, any tear or rupture allows a large volume of blood to enter the pericardial cavity, which causes cardiac tamponade.15,19 Ascending aortic aneurysms may rupture into the mediastinum and pleural cavities; if they involve the coronary arteries or aortic valve, acute aortic incompetence will occur.15 The branches of the aortic arch supply the head and upper limbs; therefore, a rupture in any of these branches can affect the pulse or BP in the upper limbs or neck, causing neurological changes, such as confusion, convulsions, and hemiplegia.20
If the descending aorta ruptures into the pleural cavity, it causes hemothorax in approximately 10% of cases—mostly in distal (but also in proximal) dissections.21,22 This typically occurs on the left side; however, it can occur on the right side following an extensive type B dissection.22 McCloy and colleagues20 found hemothorax in 6% of patients with thoracic aneurysm dissections.
Imaging Studies
Chest radiographs may show a widened mediastinum, a mediastinal mass, or indicate complications, such as a hemothorax. CT scans may demonstrate the degree of vertical extension of a descending aneurysm or type B dissections. The typical CT appearance reveals an intimal flap and a contrast between the true and false lumen. Magnetic resonance imaging provides highly detailed images that can pinpoint the areas of dissection.
Management
Aortic aneurysm and dissection can be treated medically or surgically. Antihypertensive treatment reduces the rate of aneurysm growth by decreasing BP and pulsatile load. Antihypertensive agents also decrease the incidence of surgery for acute type B dissections and reduce the rate of aortic dilatation and the frequency of subsequent hospital admissions.23 Patients with a symptomatic or large (>6 cm) aneurysm have an increased risk of aortic rupture, so elective surgery should be considered.5 Type A dissections are a surgical emergency because of the risk of cardiac tamponade. Surgery is also indicated in any dissection with an increasing aortic diameter or complications, such as hemothorax.23
Aneurysm Outcomes
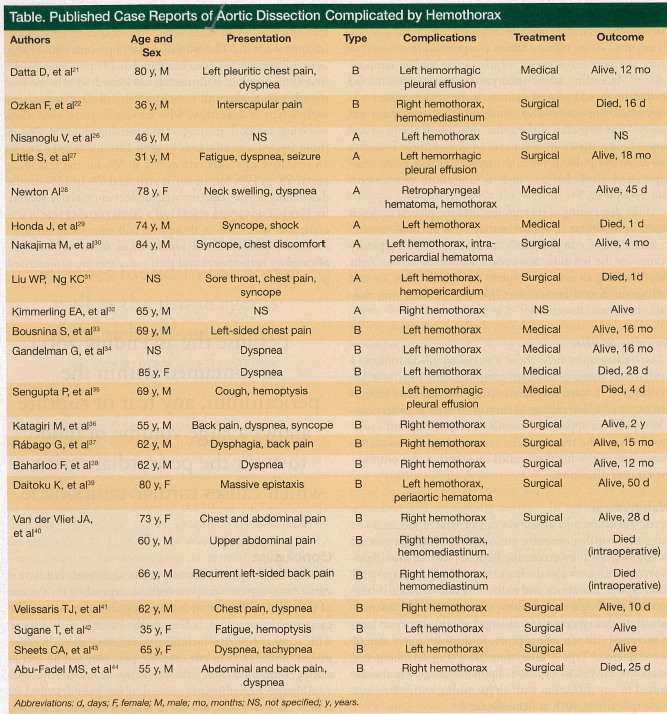
Thoracic aortic aneurysms occur more frequently in elderly women, who have an increased risk of aneurysm rupture and a higher mortality rate than men.5,11 Some studies found the mortality rates of ruptured aortic aneurysms to be as high as 94% to 100%.4,24 Bickerstaff and colleagues4 found a median interval of 2 years from diagnosis of thoracic aortic aneurysm to aneurysm rupture. Aortic dissection rupture occurred in 95% of patients, whereas nondissecting aneurysms ruptured in 51%. They also found an overall 5-year survival rate of 13%; 7% in those with aortic dissection and 19.2% in those without.4 The mortality rate in persons with type A aortic dissection has been estimated at 1% per hour for the first 48 hours, and, if untreated, can exceed 80% in the first month.8 Bergholm and associates25 found that, in patients with a type B dissection, 64% survived over 1 year when receiving medical treatment compared with only 7% in those treated urgently with surgery. Elective surgery carries an operative mortality rate of 3% to 5% for the ascending aorta, 6% to 19% for the aortic arch, and 6% to 12% for the descending aorta.5 Patients who underwent elective surgery for thoracic aneurysm repair had a 30-day fatality rate of 8% compared with 57% in those who had emergency surgery.5 Previously published case reports of aortic dissection complicated by hemothorax and their outcomes are summarized in the Table.21,22,26-44
Conclusion
Patients with ruptured thoracic aortic aneurysms can have a variety of symptoms on presentation, depending on the site of the rupture. Patients with dissecting aneurysms can suffer catastrophic events, including death. Patients may present with acute symptoms, including severe chest pain. In older people, however, as in our case, the pain may not be excruciating; thus, mild chest pain should not be underestimated.
Although hemothorax is unusual, it has been described in several cases as a complication of a thoracic aortic dissection rupture. A patient with a hemothorax on presentation, especially in combination with a significant drop in hemoglobin level, should lead to a high index of suspicion of a ruptured thoracic aortic dissection. The usual clues on chest radiographs, such as a widened mediastinum and abnormal aortic silhouettes, can be obscured by the opacification caused by the hemothorax.21
Aortic dissection has a high mortality rate; thus, early diagnosis and management are crucial. In our case, the diagnosis was delayed because the patient’s hypotension was incorrectly interpreted as being caused by sepsis despite no initial pyrexia or any subsequent positive cultures, and the drop in his hemoglobin level was not thoroughly investigated. In addition, the patient was inappropriately given anticoagulation agents due to the suspected diagnosis of MI. Therefore, as hemothorax is a recognized presentation of aortic dissection, this diagnosis should be considered in unexplained cases of hemorrhagic pleural effusions.27,45
The authors report no relevant financial relationships.
References
1. Upchurch GR, Schaub TA. Abdominal aortic aneurysm. Am Fam Physician. 2006; 73(7):1198-1204.
2. Young B, Heath JW. Wheater’s Functional Histology. 4th ed. United Kingdom: Churchill Livingstone; 2000:148.
3. Kumar P, Clark M. Clinical Medicine. 4th ed. Philadelphia, PA: W.B. Saunders; 1998:807-809.
4. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aortic aneurysms: a population-based study. Surgery. 1982;92(6):1103-1108.
5. Clouse WD, Hallett JW, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA. 1998;280(22):1926-1929.
6. Svensjö S, Bengtsson H, Bergqvist D. Thoracic and thoracoabdominal aortic aneurysm and dissection: an investigation based on autopsy. Br J Surg. 1996;83(1):
68-71.
7. Elefteriades JA. Thoracic aortic aneurysm: reading the enemy’s playbook. Yale J Biol Med. 2008;81(4):175-186.
8. Patel HJ, Deeb GM. Ascending and arch aorta: pathology, natural history and treatment. Circulation. 2008;118(2):188-195.
9. Ramanath VS, Oh JK, Sundt TM 3rd, Eagles KA. Acute aortic syndromes and thoracic aortic aneurysm. Mayo Clin Proc. 2009;84(5):465-481.
10. Judge DP, Dietz HC. Marfan’s syndrome. Lancet. 2005;366(9501):1965-1976.
11. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):
897-903.
12. Clouse WD, Hallett JW, Schaff HV, et al. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc. 2004;79(2):176-180.
13. Pate JW, Richardson RL, Eastridge CE. Acute aortic dissection. Am J Surg. 1976; 42(6):395-404.
14. Benouaich V, Soler P, Gourraud PA, Lopez S, Rousseau H, Marcheix B. Impact of meteorological conditions on the occurrence of acute type A aortic dissections. Interact Cardiovasc Thorac Surg. 2010;10(3):403-406.
15. Snell RS. Clinical Anatomy by Systems. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:95-98.
16. Tamori Y, Akutsu K, Kasai S, et al. Coexistent true aortic aneurysm as a cause of acute aortic dissection. Circ J. 2009;73(5):822-825.
17. Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Shumway NE. Management of acute aortic dissections. Ann Thorac Surg. 1970;10:237-247.
18. DeBakey ME, Henly WS, Cooley DA, Morris GC Jr, Crawford ES, Beall AC Jr. Surgical management of dissecting aneurysms of the aorta. J Thorac Cardiovasc Surg. 1965;49:130-149.
19. Gray H. Anatomy of the Human Body. 20th ed. Philadelphia, PA: Lea & Febiger; 1918.
20. McCloy RM, Spittell JA Jr, McGoon DC. The prognosis in aortic dissection (dissecting aortic hematoma or aneurysm). Circulation. 1965;31:665-669.
21. Datta D, Kanathur N, Lahiri B. Ruptured thoracic aortic dissection presenting as opacified left hemothorax. Conn Med. 2004;68(6):371-374.
22. Ozkan F, Akpinar E, Serter T, Ozyüksel A, Hazirloan T. Ruptured type B aortic dissection presenting with right hemothorax. Diagn Interv Radiol. 2008;14(1):6-8.
23. Genoni M, Paul M, Jenni R, Graves K, Seifert B, Turina M. Chronic beta-blocker therapy improves outcome and reduces treatment costs in chronic type B aortic dissection. Eur J Cardiothoracic Surg. 2001;19(5):606-610.
24. Johansson G, Markström U, Swedenborg J. Ruptured thoracic aortic aneurysms: a study of incidence and mortality rates. J Vasc Surg. 1995;21(6):985-988.
25. Bergholm U, Hallén A. Dissecting aneurysm of the descending thoracic aorta. Surgical or medical treatment? Scand J Thorac Cardiovasc Surg. 1984;18(1):45-47.
26. Nisanoglu V, Erdil N, Battaloglu B. Complete left-sided absence of the pericardium in association with ruptured type A aortic dissection complicated by severe left hemothorax. Tex Heart Inst J. 2005;32(2):241-243.
27. Little S, Johnson J, Moon BY, Mehta S. Painless left hemorrhagic pleural effusion: an unusual presentation of dissecting ascending aortic aneurysm. Chest. 1999;116(5):1478-1480.
28. Newton AI. Spontaneous retropharyngeal hematoma: an unusual presentation of thoracic aortic dissection. J Emerg Med. 2006;31(1):45-48.
29. Honda J, Yamamoto S, Wada H, Hiramoto A, Kuroki K, Okeda R. Ruptured proximal aorta after operation for type A dissection presenting as opacified left hemothorax; report of a case [in Japanese]. Kyobu Geka. 2008;61(5):398-402.
30. Nakajima M, Tsuchiya K, Naito Y, Inoue H, Kobayashi K, Mizutani E. Partial pericardial defect associated with ruptured aortic dissection of the ascending aorta: a rare feature presenting severe left hemothorax without cardiac tamponade. Ann Thorac Surg. 2004;77(3):1066-1068.
31. Liu WP, Ng KC. Acute thoracic aortic dissection presenting as sore throat: report of a case. Yale J Biol Med. 2004;77(3):53-58.
32. Kimmerling EA, Smith JK, Tenholder MF. Mediastinal mass with right pleural effusion. South Med J. 1993;86(10):1160-1163.
33. Bousnina S, Zendah I, Marniche K, et al. Left hemothorax caused by aortic dissection [in French]. Rev Pneumol Clin. 2007;63(2):119-122.
34. Gandelman G, Barzilay N, Krupsky M, Resnitzky P. Left pleural hemorrhagic effusion: a presenting sign of thoracic aortic dissecting aneurysm. Chest. 1994;106(2):636-638.
35. Sengupta P, Mitra B, Saha K, Maitra S, Pal J, Sarkar N. Descending thoracic aortic aneurysm presenting as left sided hemorrhagic pleural effusion. J Assoc Physicians India. 2007;55:297-300.
36. Katagiri M, Takahashi M. Right hemothorax: an unusual presentation of ruptured aortic dissection. J Cardiovasc Surg (Torino). 1991;32(1):135-136.
37. Rábago G, Martín-Trenor A, López-Coronado JL. Chronic aneurysm of the descending thoracic aorta presenting with right pleural effusion and left phrenic paralysis. Tex Heart Inst J. 1999;26(1):96-98.
38. Baharloo F, Verhelst R, Collard P, Pieters T. Rupture of aortic aneurysm with right-sided hemothorax. Eur Respir J. 1999;13(2):465-467.
39. Daitoku K, Takahashi K, Sudo T. Ruptured thoracic aortic aneurysm presenting as massive epistaxis; report of a case [in Japanese]. Kyobu Geka. 2004;57(5):398-401.
40. Van der Vliet JA, Heijstraten FMJ, Van Roye SF, Buskens FG. Spontaneous right hemothorax secondary to aortic rupture. Eur J Vasc Surg. 1994;8:634-638.
41. Velissaris TJ, Lloyd CT, Ohri SK. Type B aortic dissection and right hemothorax. Asian Cardiovasc Thorac Ann. 2002;10(2):197.
42. Sugane T, Takahashi N, Koura T, et al. A case of tuberculous aneurysm of the aorta. Kekkaku. 2000;75(10):589-593.
43. Sheets CA, Janz TG. Ruptured thoracic aneurysm presenting as dyspnea and hypotension. Ann Emerg Med. 1988;17(7):718-721.
44. Abu-Fadel MS, Gibbson MF, Michel LB, Peyton MD, Sivaram CA. Right sided hemothorax: an uncommon manifestation of type B aortic dissection (descending aortic dissection). Chest. 2004;126(4):958S.
45. Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122(1):311-328.