
Diagnosing a Large Facial Growth in an Elderly Woman
 A 94-year-old woman with a large growth on her face presented to my office (Figure). Approximately 4 months earlier, the patient noticed a <1-cm pinkish nodule on her left cheek. For approximately 1 month, the size and color of the lesion remained the same; however, it gradually became darker and grew to 7 x 8 cm. Although the patient felt no sensitivity to the nodule, it began to worry her family members, who brought her in for an evaluation.
A 94-year-old woman with a large growth on her face presented to my office (Figure). Approximately 4 months earlier, the patient noticed a <1-cm pinkish nodule on her left cheek. For approximately 1 month, the size and color of the lesion remained the same; however, it gradually became darker and grew to 7 x 8 cm. Although the patient felt no sensitivity to the nodule, it began to worry her family members, who brought her in for an evaluation.
One week later, I partially excised the lesion and sent the biopsy to a laboratory for further analysis. Upon further investigation, the patient admitted to having an extensive history of unprotected sun exposure. She grew up in Florida and often swam at the beach without using any type of sunscreen or ultraviolet protection. The patient’s reported medications included escitalopram, diltiazem, artificial tears, calcium tablets, senna, acetaminophen, and amitriptyline.
Based on the case description and the photograph, what is your diagnosis?
A. Benign fibrous histiocytoma
B. Dermatofibrosarcoma protuberans
C. Atypical fibroxanthoma
D. Malignant melanoma
E. Squamous cell carcinoma
F. Basal cell carcinoma
[Click next page for answer and discussion>>]
Diagnosis: Atypical fibroxanthoma (C)
Discussion
Atypical fibroxanthoma presents as a tumor on the face or neck, and it is commonly seen in elderly patients exposed to high amounts of ultraviolet light with little or no sun protection.1-3 It is described as a low-grade sarcoma, usually measuring 1 to 2 cm in length. At first, it appears as a nodule, but it quickly propagates to become brusque and ulcerated. Although specific to sun-exposed areas, an uncommon variant exists where the sarcoma can appear on skin that is free from sun damage. A few cases of atypical fibroxanthoma have been observed in children with xeroderma pigmentosum, a genetic disease in which an individual lacks the ability to repair tissue damaged by ultraviolet light. Atypical fibroxanthoma rarely metastasizes.4,5
Pathology Findings
The microscopy image of the case patient’s skin biopsy was consistent with a diagnosis of atypical fibroxanthoma, showing cellular dermal proliferation of pleomorphic atypical spindle cells with admixed mononuclear cells, multinucleated cells, and foam cells. Immunohistochemical staining was positive for CD markers 10 and 68, but was negative for S100 and cytokeratin.
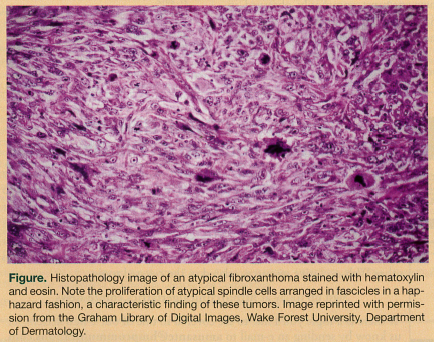
On histopathology, atypical fibroxanthomas generally show a proliferation of large, fibrocytic, spindle-shaped and anaplastic or polygonal cells arranged in fascicles in a disorderly pattern (Figure). There is also often an increased number of mitotic figures.
Treatment of Atypical Fibroxanthoma
Treatment of atypical fibroxanthoma typically entails complete excision of the nodule, as was done for the case patient. In cases of recurrence, Mohs micrographic surgery may be appropriate due to its high reliability of complete tumor removal and tissue-conserving property.
Ruling Out the Other Diagnoses
The differential diagnoses for atypical fibroxanthoma include benign fibrous histiocytoma, dermatofibrosarcoma protuberans, malignant melanoma, squamous cell carcinoma, and basal cell carcinoma.
Benign fibrous histiocytoma. Benign fibrous histiocytomas, also called dermatofibromas, are mobile, hard papules (rounded bumps) that may appear in a variety of colors, but are usually brownish to tan.6 These skin tumors often measure <2 cm and may dimple on compression. A common site of occurrence is the legs, generally in women between the ages of 20 and 50 years. Although their etiology is unclear, they have been associated with trauma and immunosuppression. Typical benign fibrous histiocytomas cause little or no discomfort, although itching and tenderness can occur. Treatment is excision, which is generally successful, with little chance of local recurrence.
Dermatofibrosarcoma protuberans. Dermatofibrosarcoma protuberans is a relatively uncommon soft tissue neoplasm that is slow-growing and locally aggressive, has a high rate of recurrence, and poses an intermediate to low risk of malignancy.7 It appears as a pink or flesh-colored nodule or lumpy keloidal plaque, often on the upper trunk. In addition to surgery, numerous cancer treatments have been used to treat dermatofibrosarcoma protuberans, including radiation and imatinib mesylate, the latter of which was specifically approved in 2006 by the US Food and Drug Administration as a treatment for adult patients with unresectable, recurrent, or metastatic lesions.
Malignant melanoma. Malignant melanoma is a neoplasm of melanocytes or of the cells that develop from melanocytes.8 These neoplasms appear as multicolored lesions with irregular borders and uneven pigmentation. They are often found on sun-damaged skin and are especially common on the back, legs, arms, and face; however, they can also occur on hidden areas of the body, such as under the fingernails, between the toes, on the genitals, and on the scalp. Although malignant melanoma can affect any age group, the risk of this deadly disease increases with age. Surgery is the definitive treatment for early-stage melanoma, with adjuvant therapies required in cases of more advanced disease.
Squamous cell carcinoma. Squamous cell carcinoma is classified as a nonmelanoma skin cancer that presents as a red-brown papule, nodule, or tumor, often indurated and ulcerated, with scaling or an even cutaneous horn.9 This cancer often occurs on the face, lower lip, or any sun-exposed area. Although it can affect any age group, its incidence increases with age. Treatment depends on the size and location of the cancer and whether it has metastasized. Treatment options may include surgical excision, curettage and electrodesiccation, cryosurgery, photodynamic therapy, radiation, and use of topical agents that contain imiquimod or 5-fluorouracil.
Basal cell carcinoma. Basal cell carcinoma, a slow-growing nonmelanoma skin cancer, has been reported to be the most common form of cancer in humans.10 These lesions are often translucent, appearing pearly or waxy, and the skin may remain flat or be only slightly raised in some cases, which can make them challenging to identify. As with other skin cancers, basal cell carcinoma tends to occur in areas that have been exposed to the sun, such as the face and neck. Metastasis is exceedingly rare, with a reported incidence of 0.028% to 0.55%.10 Although basal cell carcinomas can occur in any age group, they are most commonly observed in individuals 50 to 80 years of age, with the median age at diagnosis being 67 ± 2.5 years.10 Basal cell carcinomas are well differentiated and cells appear histologically similar to basal cells of the epidermis. Treatment is similar to that of squamous cell carcinoma.
The author reports no relevant financial relationships.
References
1. Loo DS, De Pietro WP, Moisa II, Tawfik B. Atypical fibroxanthoma of the cheek: a case report. Cutis. 1993;51(1):47-48.
2. Rice CD, Gross DJ, Dinehart SM, Brown HH. Atypical fibroxanthoma of the eyelid and cheek. Arch Ophthalmol. 1991;109(7):922-923.
3. Skoulas IG, Price M, Andrew JE, Kountakis SE. Recurrent atypical fibroxanthoma of the cheek. Am J Otolaryngol. 2001;22(1):73-75.
4. Zalla MJ, Randle HW, Brodland DG, et al. Mohs surgery vs wide excision for atypical fibroxanthoma: follow-up. Dermatol Surg. 1997;23(12):1223-1224.
5. Ang GC, Roenigk RK, Otley CC, Kim Phillips P, Weaver AL. More than 2 decades of treating atypical fibroxanthoma at Mayo Clinic: what have we learned from 91 patients? Dermatol Surg. 2009;35(5):765-772.
6. Pernick N. Benign fibrous histiocytoma (superficial). www.pathologyoutlines.com/topic/softtissuebfh.html. Accessed April 27, 2012.
7. Chen CS J, Siegel DM. Dermatofibrosarcoma protuberans. http://emedicine.medscape.com/article/
1100203-overview. Accessed April 27, 2012.
8. Tan WW. Malignant melanoma. http://emedicine.medscape.com/article/280245-overview. Accessed April 27, 2012.
9. PubMed Heath. Squamous cell carcinoma. www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001832.
Accessed April 27, 2012.
10. Bader RS. Basal cell carcinoma. http://emedicine.medscape.com/article/276624-treatment. Accessed April 27, 2012.