
Diagnosing the Cause of Progressive Dyspnea in an Elderly Man
A frail 78-year-old man with a medical history significant for smoking, chronic obstructive pulmonary disease (COPD), and peripheral vascular disease presented to the hospital with a chief concern of subacute, progressive dyspnea. This was preceded by weakness, anorexia, and weight loss. He did not have any coughing, wheezing, chest pain, lower limb edema, paroxysmal nocturnal dyspnea, orthopnea, fevers, chills, or night sweats. He was not on any inhaler therapy at home.
His initial vital signs were significant for a heart rate of 105 beats per minute, blood pressure of 104/76 mm Hg, and an oxygen saturation level of 93% on room air. Significant physical examination findings included cachexia and a sacral ulcer. His lungs showed vesicular breath sounds with crackles in the left upper lobe. Laboratory values indicated no leukocytosis, and his electrolyte panel, blood urea nitrogen level, and creatinine level were all within normal limits. A chest radiograph (Figure 1) and computed tomography (CT) scan of his chest (Figure 2) showed significant findings.
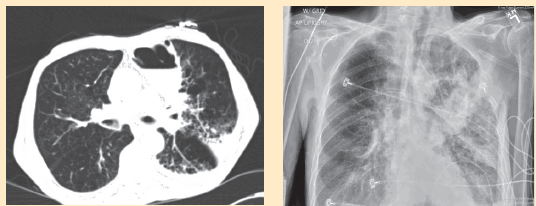
Figure 1. Chest radiograph shows a focal area of consolidation in the left lung.
Figure 2. Computed tomography scan of the patient’s chest shows an air-fluid level with a surrounding infiltrate.
Based on the clinical presentation and the imaging findings, what is your diagnosis?
A. Infected emphysematous bulla
B. Lung abscess
C. Hemorrhagic bulla
D. Congestive heart failure
E. Malignancy
Visit Annals of Long-Term Care: Clinical Care and Aging to find out the answer and a discussion>>