
Diabetes Agents in the Elderly: An Update of New Therapies and a Review of Established Treatments
This article is the third in a continuing series on diabetes in the elderly. The second article in the series, “Quality Improvement in the Diagnosis and Management of Diabetes Mellitus in Older Adults,” was published in the May issue of the Journal. The remaining articles in the series will discuss such topics as insulin in the management of elderly patients with diabetes, the role of exercise and dietary supplements in the management of diabetes, and microvascular and macrovascular complications of diabetes.
Introduction
Individuals 65 years and older currently account for 12.4% of the U.S. population.1 By 2040, this percentage is predicted to exceed 20%.2 In the United States, diabetes affects 23.6 million people, or 7.8% of the population. In those over age 60 years, it affects 12.2 million, or 23.1% of people in this age group. Estimated direct and indirect diabetes costs in the United States are more than $174 billion annually.3 Despite the multiple classes of available diabetes medications, the majority of persons with type 2 diabetes are unable to maintain long-term glycemic control.4 Fewer than half of U.S. adults with type 2 diabetes mellitus reach an HbA1c level of less than 7%.5 With the morbidity and mortality related to diabetes and diabetes-related complications well established, having a better understanding of these in the elderly becomes increasingly important.
Recent years have brought many new classes of diabetic medications. The objective of this review is to delineate the safety and efficacy of those medications in the elderly, as well as to review the established medications. The data in the elderly are limited depending on the drug studied. This article will focus on the new and established oral agents, as well as new noninsulin injectable medications. An upcoming article in the next issue of Clinical Geriatrics will focus on the new insulin treatment options.
New Classes of Diabetes Medications
Incretin Mimetics
Incretins are gastrointestinal (GI) hormones that increase the amount of insulin released from the beta cells of the pancreas after eating, even before blood glucose levels become elevated. The two main incretin molecules are glucagon-like peptide-1 (GLP-1) and gastric inhibitory peptide (also known as glucose-dependent insulinotropic peptide [GIP]). Additionally, incretins slow the rate of absorption of nutrients into the bloodstream by reducing gastric emptying and may directly reduce food intake. By doing so, they also inhibit glucagon release from the alpha cells of the pancreas.5-7
Both GLP-1 and GIP are rapidly inactivated by the enzyme dipeptidyl peptidase-4.6,8,9 Incretin action depends on glucose concentration, and its function ceases when the serum glucose level is less than 55 mg/dL.5 This is an inherent benefit of the drug, in that it facilitates a glucose-mediated insulin release with less risk of hypoglycemia. GLP-1 is secreted from the L cells of the intestinal mucosa, in response to ingestion of mixed meals or glucose.6,8,9 Actions of GLP-1 include stimulating insulin secretion, inhibiting glucagon secretion and hepatic glucose output, decreasing gastric emptying and motility, and decreasing appetite and food intake.8,9
In terms of appetite, GLP-1 agonists increase serotonin release in the hypothalamus, and their central anorectic effects could be partially mediated by this.10 In addition, GLP-1 receptor has anorexigenic and fat-reducing properties, as opposed to ghrelin, which is a potent orexigenic and adipogenic hormone, and strongly influences fat deposition and generation of hunger. Incretins reduce the levels of ghrelin by up to 74% in fasted rats, which may explain reduced food intake.11
The first drug in this class on the market was exenatide. Exendin-4 is a biologically active peptide discovered in the lizard Heloderma suspectum (Gila monster) venom.12 It shares about 50% of its amino acid sequence with mammalian GLP-1.6 Exenatide is a synthetic form of this peptide and is the first GLP-1–based therapy to be approved in the United States by the Food and Drug Administration (FDA) for the treatment of type 2 diabetes. The half-life of exenatide is longer than that of intact GLP-1 (1-3 min), and it is a potent agonist of the mammalian GLP-1R.6 It is the first available incretin mimetic indicated for the treatment of type 2 diabetes in patients taking metformin (a biguanide), a sulfonylurea, or a thiazolidinedione.12 The glucoregulatory effects of exenatide are achieved through multiple mechanisms, including the enhancement of glucose-dependent insulin secretion, suppression of postprandial glucagon secretion, slowing of gastric emptying, and reduction in food intake.12-14 Studies show that patients receiving GLP-1 analogues have statistically significant decline in A1C as compared with placebo, and patients receiving exenatide are more likely to achieve an A1C of less than 7%.5
The weight loss observed with GLP-1 analogues was statistically significant in trials that reported data on weight.13-17 The weight loss was more pronounced when exenatide was compared with insulin.16 Weight loss with exenatide was progressive and dose-dependent.13-16
Severe hypoglycemia (requiring assistance) was rare with GLP-1 analogues, reported in only five of 2781 patients treated with exenatide. Those patients also received sulfonylureas.15,16 Hypoglycemia peaked during initiation of therapy with exenatide, and then decreased over time.13,15,16 The risk of hypoglycemia was similar between exenatide versus insulin.16
The most frequently reported adverse events with exenatide are dose-dependent nausea and vomiting, occurring in as many as 57% (nausea) and 17% (vomiting) of patients treated with exenatide. Nausea is reported as mild to moderate, increasing during the initial eight weeks and declining thereafter. Dose titration tends to attenuate nausea.10,11,13,14 Diarrhea is also more pronounced with exenatide versus placebo (risk ratio, 2.2; 95% confidence interval [CI], 1.7-2.9).5
Exenatide is administered as a subcutaneous injection. Therapy should be initiated at 5 mcg per dose administered twice daily at any time within the 30-60–minute period before morning and evening meals (or before the patient’s two main meals of the day, approximately ≥ 6 hr apart). Based on clinical response, the dose can be increased to 10 mcg twice daily after 1 month of therapy. It is not recommended in patients with end-stage renal disease or severe renal impairment (creatinine clearance < 30 mL/min/1.73m2). In addition, patients on dialysis experienced increased GI side effects. Exenatide is predominately eliminated by glomerular filtration with subsequent proteolytic degradation. The terminal half-life (2.4 hr) of exenatide is independent of dose, age, gender, race, and weight of the patient (obesity vs nonobesity).18
Dose-dependent nausea and vomiting are the most frequently reported adverse effects of exenatide versus placebo. This could be a limiting factor when using this medication in elderly patients with diabetes. One needs to consider, however, that there is a dose-dependent attenuation of that adverse effect. Caution should be exercised when using exenatide with sulfonylurea hypoglycemic medications to avoid the risk of hypoglycemia in the elderly. There have been 36 postmarketing reports of acute pancreatitis in patients taking exenatide. Pancreatitis should be considered in patients with abdominal pain, and exenatide should be discontinued in such patients. The drug should not be restarted if pancreatitis is confirmed. In an elderly population, this is an important consideration, as they are often taking many medications that may also predispose to pancreatitis.
Liraglutide is a newly-approved, long-acting, acylated GLP-1 analogue with a half-life of 14 hours.8,17 It is administered once daily, independent of the timing of meals. Studies show that liraglutide can provide adequate glycemic control in patients with type 2 diabetes. It also results in modest weight loss and favorable changes in body composition comparable to that produced by metformin.8
It has been noted in animal studies that subcutaneous administration of liraglutide for an extended period of time (200 mg/kg twice daily for 10 days) caused significant weight loss (up to 15% of initial body weight) in normal rats and in rats with hypothalamus-induced obesity, primarily because of anorectic effects.8 In addition, liraglutide has been associated with a significant reduction in weight (2.0-2.5 kg) when compared with placebo. It also showed similar efficacy in reducing the A1C as compared with glimepiride or metformin.5
The key warning about liraglutide includes an increased risk of C-cell tumors of the thyroid in rodent models. Thus, its use is contraindicated in patients with a personal or family history of medullary thyroid cancer or in patients with multiple endocrine neoplasia syndrome type 2. Additionally, it should be used with caution in patients with a history of pancreatitis. The most common adverse events are nausea, vomiting, and diarrhea. These occur at rates of 10-40%. While weight loss caused by liraglutide may be a limiting factor in elderly malnourished patients, it may be a good option in older patients who are obese due to a favorable profile in terms of hypoglycemia.
Dipeptidyl Peptidase-4 Inhibitors
Dipeptidyl peptidase-4 (DPP-4) inhibitors enhance levels of active incretin hormones. Both GLP-1 and GIP are rapidly inactivated by the enzyme DPP-4. DPP-4 inhibitors block this inactivation, thereby increasing active incretin levels and enhancing incretin effects.19,20 Sitagliptin and saxagliptin are approved in the United States. They are oral, once-daily, potent, and selective DPP-4 inhibitors. Sitagliptin inhibits plasma DPP-4 activity more than 80% over 24 hours with single doses of greater than 100 mg. In patients with type 2 diabetes, this inhibition produces two- to threefold increases in active GLP-1 and GIP levels, reduces plasma glucagons levels, and reduces glycemic excursion following an oral glucose tolerance test.20
Studies show that DPP-4 inhibitors lowered HbA1C with similar efficacy both as monotherapy or add-on therapy.5 Patients receiving DPP-4 inhibitors were more likely to achieve an HbA1c of less than 7% as compared with placebo (43% vs 17%). There was a small increase in weight with DPP-4 inhibitors as compared with placebo (weighted mean difference, 0.5 kg; 95% CI, 0.3-0.7 kg). Sitagliptin had a favorable weight profile as compared with glipizide (–2.5 kg vs 1.0 kg, respectively). Severe hypoglycemia was reported in only two patients receiving DPP-4 inhibitors.5 There was no increased risk of GI side effects (nausea, vomiting, diarrhea, and abdominal pain) when comparing DPP-4 inhibitors with placebo; overall, they were very well tolerated. Available data reveal an increased risk of nasopharyngitis (6.4% for DPP-4 inhibitor vs 6.1% for comparator), which is more evident with sitagliptin as compared with other DPP-4 inhibitors, and an increased risk of urinary tract infection UTI). Headache was also reported more commonly with DPP-4 inhibitors.5
There have been 88 postmarketing case reports of acute pancreatitis in patients using sitagliptin. Similar to the incretins, pancreatitis should be considered in patients with abdominal pain and the medication discontinued. It is not known whether the issue of pancreatitis is a class effect of GLP-1–mediated drugs.
When prescribing DPP-4 inhibitors for the elderly, caution should be exercised regarding the potential side effect of increased risk of UTI and nasopharyngitis. Elderly patients with diabetes often have increased morbidity related to these conditions at baseline. As DPP-4 inhibitors do not cause significant weight loss, they may be preferred over GLP-1 analogues in malnourished elderly patients. Because there is a need for dosage adjustment based upon renal function, assessment of renal function is recommended prior to initiation of sitagliptin, and periodically thereafter. When sitagliptin is used in combination with a sulfonylurea, a lower dose of sulfonylurea may be required to reduce the risk of hypoglycemia.21
Amylin Analogues
Amylin is a 37 amino acid peptide hormone that is co-secreted from the beta cells of the pancreas along with insulin in response to meals.22 Thus, amylin secretion is virtually absent in type 1 diabetes. Patients with type 2 diabetes have relative amylin deficiency.23
Pramlintide. Pramlintide is an injectable synthetic analogue of amylin. It was approved by the FDA in 2005 for use in both type 1 and insulin-dependent type 2 diabetes. In patients with type 2 diabetes, it is used in addition to premeal insulin. It is not approved for use with exenatide. Pramlintide acts through amylin receptors located in nucleus accumbens and dorsal vagal complex, which provide parasympathetic motor innervation to the GI tract. Activation of neuronal amylin receptors reduces food intake, depresses GI motility, and promotes satiety.24 Amylin also suppresses postprandial glucagon secretion by an incompletely understood neuroendocrine pathway.25
Pramlintide is injected subcutaneously, has a half-life of 29 minutes, and is primarily eliminated via the kidneys. The dose does not need to be adjusted for the elderly or patients with renal or hepatic impairment. There are no data available on the safety in patients on dialysis with end-stage renal disease. Therapy with pramlintide is started at a low dose to reduce incidence of nausea, and titrated up every three to seven days to the target dose.
Benefits of pramlintide are reduction in HbA1c by 0.2-0.6%,26-28 reduction of two-hour postprandial glucose and potential weight loss (as compared to weight gain commonly seen with insulin, sulfonylureas, and thiazolidinediones), and reduction in total daily insulin dose. Whitehouse et al26 showed that weight loss induced by pramlintide may be transient, which needs to be further investigated by a long-term, randomized, controlled trial.
The primary side effects of pramlintide include nausea, hypoglycemic episodes, extra daily subcutaneous injections in addition to insulin, increased cost of therapy, and decreased absorption of other oral medications secondary to slowing of gastric emptying. Rate of nausea varied between 10% and 59%.26,27,29 In most patients, nausea, vomiting, and anorexia tend to resolve following the first two to eight weeks of therapy, but no data are published to support this reduction in nausea. The rate of hypoglycemia is increased during the first four weeks of therapy.27,30 The manufacturer recommends reducing the dose of premeal insulin by 50% when starting pramlintide.31 Pramlintide does not appear to reduce the glucagon and other counterregulatory hormone response to hypoglycemia.32
Pramlintide is contraindicated in patients with gastroparesis, frequent hypoglycemic episodes, hypoglycemic unawareness, and hypersensitivity to pramlintide, metacresol, D-mannitol, acetic acid, or sodium acetate. Pramlintide may delay the absorption of oral medications. Therefore, it is advised to take oral medications 1 hour before or 2 hours after the dose of pramlintide, which can be troublesome in elderly patients with diabetes, who are usually taking multiple medications.
Pramlintide has gained popularity as a result of its relatively few contraindications, minimal risk of hypoglycemia, and potential for weight loss, but its role in the elderly diabetic population is unclear. Multiple daily injections, nausea, interaction with oral medications, and episodes of hypoglycemia mandate increased alertness, compliance, frequent glucose monitoring, and constant supervision. This may complicate its use in the elderly population. On the other hand, it might be beneficial in motivated elderly persons with diabetes who have good functional status, limited comorbidities, life expectancy greater than 10 years, and preserved cognitive function, who are poorly controlled with insulin regimen and/or are frustrated by insulin-induced weight gain. Because the pramlintide dose is not affected by liver disease, kidney disease, or age, it might be worthwhile to consider pramlintide as an adjuvant to insulin.
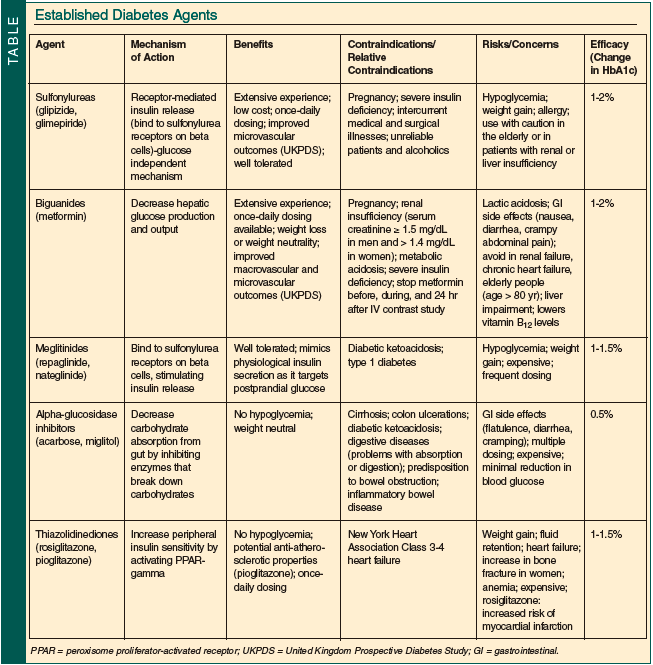
Established Diabetes Agents
In addition to the newer agents noted above, pharmacological treatment of diabetes includes the spectrum of oral medication, including sulfonylureas, meglitinides, biguanides, alpha-glucosidase inhibitors, and thiazolidinediones. These established drug classes will be reviewed briefly here (Table).
Insulin Sensitizers with Predominant Action in the Liver: Biguanides
Metformin is the only biguanide available in the United States, marketed since 1995. The precise mechanism of action of metformin is unknown. It works to reduce hepatic insulin resistance, and, thereby, gluconeogenesis and glucose production. Metformin reduces hepatic gluconeogenesis, and enhances post-receptor insulin sensitivity and insulin-mediated glucose disposal. When used alone, it does not cause hypoglycemia. It is generally taken at least twice daily, although a sustained-release formulation is now available.33
In the United Kingdom Prospective Diabetes Study,34 patients randomly assigned to metformin had improvements in microvascular complications similar to those randomly assigned to insulin and sulfonylurea, and demonstrated a reduction in diabetes-related deaths and myocardial infarction. The beneficial effect of metformin is supported by different observations, such as metformin-associated modest reductions in low-density lipoprotein cholesterol, triglycerides, blood pressure, and procoagulant factors.35
Biguanides are not associated with significant risk of hypoglycemia, as they do not increase insulin levels. The most common adverse events are GI-related: nausea; diarrhea; and crampy abdominal pain. The GI distress can be minimized by starting with a low dose once daily with meals and titrating upward slowly. Sustained-release metformin is associated with fewer upper GI symptoms but can increase the frequency of diarrhea. The vast majority of patients tolerate metformin very well (at least 90% of patients).35
Metformin is associated with less weight gain and, in some studies, modest mean weight loss. The most concerning side effect of metformin is lactic acidosis, which is quite rare and occurs almost exclusively in patients who are at high risk of developing lactic acidosis even without metformin therapy. Metformin is cleared by the kidney; hence, it is contraindicated in patients with renal insufficiency. It should not be used in males with a serum creatinine of 1.5 mg/dL or higher, and in females of higher than 1.4 mg/dL. Metformin is also contraindicated in patients with congestive heart failure requiring treatment, in those with hepatic insufficiency, and in the setting of alcohol abuse. Caution is required in elderly people, patients with acute illness or poorly controlled chronic illness, and in the setting of simultaneous treatment with nephrotoxic drugs.36
Insulin Sensitizers with Predominant Action in Peripheral Insulin-Sensitive Tissues: Thiazolidinediones
The thiazolidinedione class of medications is believed to work through binding and modulation of the activity of a family of nuclear transcription factors, termed peroxisome proliferator-activated receptors (PPARs). Current available medications in this class are pioglitazone and rosiglitazone. Because of their effects on improving insulin resistance, the thiazolidinediones have gained popularity, currently representing 25% of all antihyperglycemic prescriptions.36
Thiazolidinediones are generally well tolerated but have the potential side effects of fluid retention, lower extremity edema, and weight gain. Cardiac status is assessed in all patients before starting these drugs. Thiazolidinediones are contraindicated in New York Heart Association Class 3-4 heart failure.35 When initiated, the patients most likely to experience edema are those with pre-existing edema. More severe edema may require adding a loop diuretic or discontinuation of therapy. Severe fluid retention resistant to diuretic therapy has been reported.35 Fluid accumulation is particularly problematic in the elderly. Despite the limitations, thiazolidinediones may be well suited for use in the elderly with normal cardiac function. Recently, there has been much discussion about the use of rosiglitazone and the risk of heart disease. These data are evolving, with further recommendations pending.
Insulin Secretagogues
Sulfonylureas. Sulfonylureas have been available since the 1950s. They have a slow onset of action and variable duration of action. There are first- and second-generation drugs available. The second-generation agents are more potent and have fewer adverse effects. Glipizide and glimepiride are the preferred drugs in this class in the elderly, as they have less hypoglycemia as compared to glyburide and can be given as a once-daily dose. Because they increase insulin secretion, they are associated with risk of hypoglycemia and weight gain, but otherwise are very well tolerated. The risk of hypoglycemia with these drugs needs to be clearly discussed with the patient upon initiation of treatment.35
Meglitinides. Repaglinide is an insulin secretagogue which has a short half-life, rapid absorption, and produces faster and briefer stimulation of insulin secretion. It is taken with each meal and provides better postprandial control. Nateglinide is structurally different from both sulfonylureas and the other meglitinides. It has a shorter duration of action than repaglinide. It is taken with meals and lowers postprandial glucose, has a very little effect on fasting glucose, and hence causes less hypoglycemia. Because of the need for multiple daily doses, and greater expense, these medications are not used as frequently as sulfonylureas.36
Carbohydrate Absorption Inhibitors: Alpha-Glucosidase Inhibitors
Inhibitors of alpha-glucosidase constitute another group of oral antidiabetic agents, which primarily influence postprandial hyperglycemia. This group includes acarbose and miglitol. Their safety profile is advantageous in the elderly, but gaseous distention and diarrhea are major side effects. These medications work by inhibiting the terminal step of carbohydrate digestion at the brush border of the intestinal epithelium, which causes shifting of carbohydrate absorption to distal intestine and delayed absorption. Their use in the United States is limited due to multiple side effects (flatulence, diarrhea, cramping), need for multiple daily dosing, cost, and only minimal reduction of blood glucose. To minimize the side effects, they should be started with a low dose once daily and increased over a period of weeks to months to the maximal dose with each meal.33,35,36
Conclusions
Management of type 2 diabetes hinges upon multiple factors, including diet modification, exercise, discontinuation of tobacco, and medical therapy. Older adults with diabetes have higher rates of comorbid conditions, functional disabilities, and are at greater risk for several common geriatric syndromes such as depression, cognitive impairment, urinary incontinence, injurious falls, and persistent pain.37 Most diabetes guidelines emphasize intensive glucose control to prevent microvascular complications. Very few guidelines are targeted toward the needs of the older population. Control of cardiovascular risk factors has a greater impact on morbidity and mortality in the elderly population than tight glycemic control alone. Approximately eight years are needed after treating diabetes with tight glycemic control to achieve a reduction in microvascular complications such as diabetic nephropathy, neuropathy, and retinopathy.34 On the other hand, the benefit of lipid and blood pressure control is seen in two to three years.38,39 Therefore, it is important to emphasize more aggressive blood pressure and lipid management, and aspirin therapy, to reduce cardiovascular end points in elderly persons with diabetes.
It is likely that intensive glucose management may be associated with reduction of hyperglycemia-related symptoms such as polyuria, polydypsia, and fatigue, and may maximize cognitive function; however, available data suggest that these shorter-term benefits may be achieved by less aggressive management of blood glucose in elderly persons with diabetes. Hence, there should be an individualized approach to the target HbA1c levels and glycemic control in this population, always with the goal of avoiding hypoglycemia. Patients with good functional capacity, few comorbidities, and life expectancy more than 10 years should have intensive glucose management with an HbA1c goal of less than 7%. At age 80 years, 70% of the elderly population has multiple chronic conditions, requiring additional medications, which increase the risk of potential side effects and drug-drug interactions.40
The addition of new agents to treat diabetes aids greatly in the armamentarium clinicians are equipped with to treat this illness. As we have evolved from being limited only to insulin and sulfonylureas, we are able to individually tailor therapy to every patient. Additionally, we are able to target different aspects of the pathophysiology of the disease, and different parts of the glucose regulation cycle. However, the newer drugs also cost more, with prescription costs for glitazones, exenatide, and sitagliptin eight to ten times those of sulfonylureas and five to seven times those of metformin.41 The mean price of a diabetes drug prescription increased from $56 in 2001 to $76 in 2007, which is in part due to the increased use of newer, more costly drugs, such as ultrashort-acting insulins ($156 in 2007), long-acting insulins ($123 in 2007), exenatide ($202 in 2007), and sitagliptin ($160 in 2007).41 This could be another limiting factor when approaching diabetes management in the elderly. Due to increased complexity of diabetes care, more combined products, and multiple medications per patient, patient education and involvement of the family remain key factors in treating older patients with diabetes. An understanding of the risks and benefits of these multiple treatment options is critical in the management of diabetes in the elderly.
The authors report no relevant financial relationships.
Dr. Arzumanyan is a third-year Internal Medicine Resident and Dr. Kant is a second-year Internal Medicine Resident, Johns Hopkins/Sinai Hospital Program in Internal Medicine, Baltimore, MD; and Dr. Thomas is Division Director, Division of Endocrinology, Sinai Hospital of Baltimore, and Associate Program Director, Johns Hopkins/Sinai Hospital Program in Internal Medicine.
References
1. American Community Survey. http://www.census.gov/acs/www/index.html. U.S. Census Bureau. Accessed May 25, 2010.
2. Morrow LA, Halter JB. Diabetes mellitus in the older adult. Geriatrics 1988;43(suppl):57-65.
3. Centers for Disease Control and Prevention. National diabetes fact sheet: General information and national estimates on diabetes in the United States, 2007. www.cdc.gov/Diabetes/pubs/pdf/ndfs_2007.pdf. Accessed May 10, 2010.
4. Koro CE, Bowlin SJ, Bourgeois N, Fedder DO. Glycemic control from 1988 to 2000 among U.S. adults diagnosed with type 2 diabetes: A preliminary report. Diabetes Care 2004;27(1):17-20.
5. Amori RE, Lau J, Pittas AG. Efficacy and safety of incretin therapy in type 2 diabetes: Systematic review and meta-analysis. JAMA 2007;298(2):194-206.
6. Drucker DJ, Nauck MA. The incretin system: Glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006;368(9548):1696-1705.
7. Doggrell SA. Is exenatide improving the treatment of type 2 diabetes? Analysis of the individual clinical trials with exenatide. Rev Recent Clin Trials 2007;2(1):77-84.
8. Feinglos MN, Saad MF, Pi-Sunyer FX, et al. Effects of liraglutide (NN2211), a long-acting GLP-1 analogue, on glycaemic control and bodyweight in subjects with type 2 diabetes. Diabet Med 2005;22(8):1016-1023.
9. Kim D, MacConell L, Zhuang D, et al. Effects of once-weekly dosing of a long-acting release formulation of exenatide on glucose control and body weight in subjects with type 2 diabetes. Diabetes Care 2007;30(6):1487-1493. Published Online: March 12, 2007.
10. Brunetti L, Orlando G, Recinella L, et al. Glucagon-like peptide 1 (7-36) amide (GLP-1) and exendin-4 stimulate serotonin release in rat hypothalamus. Peptides 2008;29(8):1377-1381. Published Online: April 20, 2008.
11. Pérez-Tilve D, González-Matias L, Alvarez-Crespo M, et al. Exendin-4 potently decreases ghrelin levels in fasting rats. Diabetes 2007;56(1):143-151.
12. Nelson P, Poon T, Guan X, et al. The incretin mimetic exenatide as a monotherapy in patients with type 2 diabetes. Diabetes Technol Ther 2007;9(4):317-326.
13. Buse JB, Henry RR, Han J, et al; Exenatide-113 Clinical Study Group. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004;27(11):2628-2635.
14. DeFronzo RA, Ratner RE, Han J, et al. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes. Diabetes Care 2005;28(5):1092-1100.
15. Kendall DM, Riddle MC, Rosenstock J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes treated with metformin and a sulfonylurea. Diabetes Care 2005;28(5):1083-1091.
16. Heine RJ, Van Gaal LF, Johns D, et al; GWAA Study Group. Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes: A randomized trial. Ann Intern Med 2005;143(8):559-569.
17. Madsbad S, Schmitz O, Ranstam J, et al; NN2211-1310 International Study Group. Improved glycemic control with no weight increase in patients with type 2 diabetes after once-daily treatment with the long-acting glucagon-like peptide 1 analog liraglutide (NN2211): A 12-week, double-blind, randomized, controlled trial. Diabetes Care 2004;27(6):1335-1342.
18. Byetta [package insert]. San Diego, CA: Amylin Pharmaceuticals, Inc; 2009. http://pi.lilly.com/us/byetta-pi.pdf. Accessed May 10, 2010.
19. Charbonnel B, Karasik A, Liu J, et al; Sitagliptin Study Group. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing metformin therapy in patients with type 2 diabetes inadequately controlled with metformin alone. Diabetes Care 2006;29(12):2638-2643.
20. Aschner P, Kipnes MS, Lunceford JK, et al; Sitagliptin Study Group. Effect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care 2006;29(12):2632-2637.
21. Januvia [package insert]. Whitehouse Station, NJ: Merck Sharp & Dohme Corp; 2010. http://www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf. Accessed May 10, 2010.
22. Koda JE, Fineman M, Rink TJ, et al. Amylin concentrations and glucose control. Lancet 1992;339(8802):1179-1180.
23. Ryan GJ, Jobe LJ, Martin R. Pramlintide in the treatment of type 1 and type 2 diabetes mellitus. Clin Ther 2005;27(10):1500-1512.
24. Sexton PM, Paxinos G, Kenney MA, et al. In vitro autoradiographic localization of amylin binding sites in rat brain. Neuroscience 1994;62(2):553-567.
25. Weyer C, Maggs DG, Young AA, Kolterman OG. Amylin replacement with pramlintide as an adjunct to insulin therapy in type 1 and type 2 diabetes mellitus: A physiological approach toward improved metabolic control. Curr Pharm Des 2001;7(14):1353-1373.
26. Whitehouse F, Kruger DF, Fineman M, et al. A randomized study and open-label extension evaluating the long-term efficacy of pramlintide as an adjunct to insulin therapy in type 1 diabetes. Diabetes Care 2002;25(4):724-730.
27. Ratner RE, Dickey R, Fineman M, et al. Amylin replacement with pramlintide as an adjunct to insulin therapy improves long-term glycaemic and weight control in type 1 diabetes mellitus: A 1-year, randomized controlled trial. Diabet Med 2004;21(11):1204-1212.
28. Hollander PA, Levy P, Fineman MS, et al. Pramlintide as an adjunct to insulin therapy improves long-term glycemic and weight control in patients with type 2 diabetes: A 1-year randomized controlled trial. Diabetes Care 2003;26(3):784-790.
29. Thompson RG, Pearson L, Kolterman OG. Effects of 4 weeks’ administration of pramlintide, a human amylin analogue, on glycaemia control in patients with IDDM: Effects on plasma glucose profiles and serum fructosamine concentrations. Diabetologia 1997;40(11):1278-1285.
30. Weyer C, Fineman MS, Strobel S, et al. Properties of pramlintide and insulin upon mixing. Am J Health Syst Pharm 2005;62(8):816-822.
31. Symlin [package insert]. San Diego, CA: Amylin Pharmaceuticals, Inc.; 2005. http://www.amylin.com/products/symlin.htm.
32. Hoogwerf BJ, Doshi KB, Diab D. Pramlintide, the synthetic analogue of amylin: Physiology, pathophysiology, and effects on glycemic control, body weight, and selected biomarkers of vascular risk. Vasc Health Risk Manag 2008;4(2):355-362.
33. Bolen S, Feldman L, Vassy J, et al. Systematic review: Comparative effectiveness and safety of oral medications for type 2 diabetes mellitus [published correction appears in Ann Intern Med 2007;147(12):887]. Ann Intern Med 2007;147(6):386-399.
34. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group [published correction appears in Lancet 1999;354(9178):602]. Lancet 1998;352(9131):837-853.
35. Inzucchi SE. Oral antihyperglycemic therapy for type 2 diabetes: Scientific review. JAMA 2002;287:360-372.
36. Nathan DM. Clinical practice. Initial management of glycemia in type 2 diabetes mellitus. N Engl J Med 2002;347:1342-1349.
37. Brown AF, Mangione CM, Saliba D, Sarkisian CA; California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes. Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc 2003;51(5 suppl guidelines):S265-S280.
38. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group [published correction appears in BMJ 1999;318(7175):29]. BMJ 1998;317(7160):703-713.
39. Haffner SM, Lehto S, Rönnemaa T, et al. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339(4):229-234.
40. Wolff JL, Starfield B. Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 2002;162(20):2269-2276.
41. Alexander GC, Sehgal NL, Moloney RM, Stafford RS. National trends in treatment of type 2 diabetes mellitus, 1994-2007. Arch Intern Med 2008;168(19):2088-2094.