
 Case 1:
Case 1:
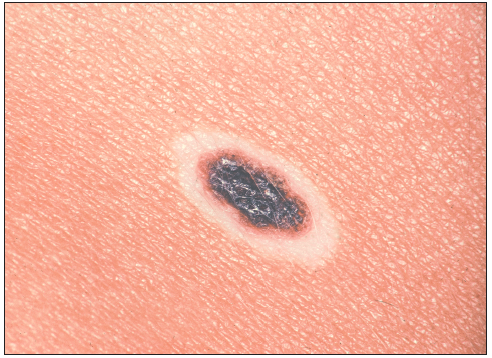
A white ring recently developed around this lesion on the upper back of a 15-year-old boy. Is there any reason for concern--and what clues would you use to suggest the need for a biopsy?
Case 1: This is a halo nevus. Halo nevi are the easiest nevi to diagnose and manage. They are also among the nevi that cause me the greatest concern. Halo nevi occur in fewer than 1% of the pediatric population, but I suspect that they are vastly underreported by patients. In Caucasians, the halo is commonly difficult to discern. The mean age of patients who present with halo nevi is said to be about 15 years. What is frightening is that approximately 20% of patients who present with halo nevi also have atypical nevi or melanoma or associated vitiligo.
I think of these lesions as nevi that develop a halo rather than as a separate variant of nevi. The typical halo nevus appears on the trunk--particularly on the upper back. Patients report that a hypopigmented halo became noticeable over several months. There is rarely any history or sign of inflammation. The halo is usually a few millimeters wide, uniform, and circumferential about a central nevus.
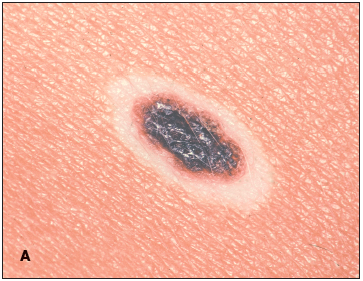 The most important aspect of the physical examination is to clearly identify the morphologic features of the central pigmented nevus. The features should be assessed as one would any pigmented lesion of the skin that is undergoing change. The color of the nevus should be even and the borders regular. The nevus itself should be central within the halo, with a clear definition to the interface between the halo and the pigmented border (A).
The most important aspect of the physical examination is to clearly identify the morphologic features of the central pigmented nevus. The features should be assessed as one would any pigmented lesion of the skin that is undergoing change. The color of the nevus should be even and the borders regular. The nevus itself should be central within the halo, with a clear definition to the interface between the halo and the pigmented border (A).
The natural history of a halo nevus is not very well documented. In my experience, the pigmented lesion within the typical halo nevus becomes lighter with time--usually in an even and predictable manner (B). This change occurs over years until the pigmentation has disappeared and the halo has repigmented. Problems occur if the regression is irregular, resulting in an unusual pigment pattern or the development of scale or other surface change.However, all degrees of regression may occur. Some lesions remain stable for years. Others progress rapidly, with simultaneous development of haloes surrounding multiple other nevi. All of these patterns may be innocent; on occasion, however, they may represent an atypical or malignant pattern-- either to the nevus itself or as a clue to changes in another nevus that may be atypical or malignant.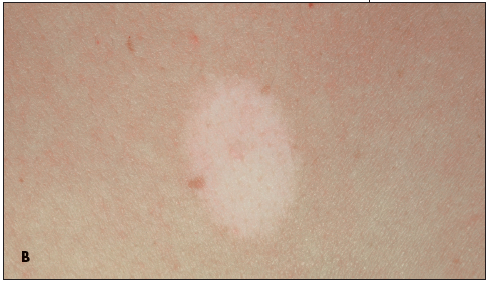
In a young child with a "typical" halo nevus, I can be reassuring. I do, however, examine all of the child's other nevi and I request an annual follow-up examination so that I can spot early changes. This is particularly important in a child who has multiple atypical nevi or who has a family history of multiple atypical nevi or malignant melanoma.
If the nevus itself exhibits any significant irregularity in pigmentation, if the pigmented area is not central within the halo, or if there is persistent erythema, I recommend removal of the nevus--along with the halo if possible.
 Case 2:
Case 2:
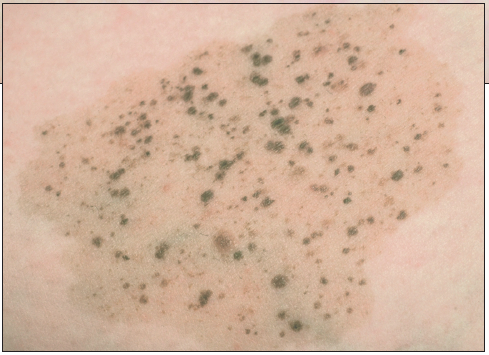
A 16-year-old girl is brought for evaluation of this pigmented lesion on her upper arm, which has been present since she was 2 years old. She asks whether it should be removed in light of her mother's recent history of malignant melanoma.
Is this lesion benign? Does it need to be removed?
Case 2: Nevus spilus or speckled lentiginous nevus is another pigmented lesion that is easy to recognize. Such lesions can sometimes be difficult to manage because there have been an increasing number of reports of the development of malignant melanoma within these nevi--although such cases are still rare. Therefore, it is becoming increasingly important to recognize these lesions and to establish a protocol for patient education and regular evaluation.
The typical nevus spilus is well demarcated and has an evenly pigmented light brown macular background. It usually measures 2 to 6 cm in diameter, but large (1 to 20 cm) lesions are not uncommon. Multiple 2 to 4-mm macular and papular pigmented lesions are randomly scattered throughout. The lesions often start out with only a few speckles; more appear during childhood. The "typical" nevus spilus can be considered benign as long as it retains this characteristic morphology. The diagnosis is almost always clinical.
The nevus is usually acquired. However, nevus spilus has also been reported in 2 of 1000 newborns as a congenital variant. Approximately 2% of schoolchildren have been noted to have such lesions. Histologically, the tan background reveals hyperplasia of the melanocytes and the smaller papules are simple nevocellular nevi.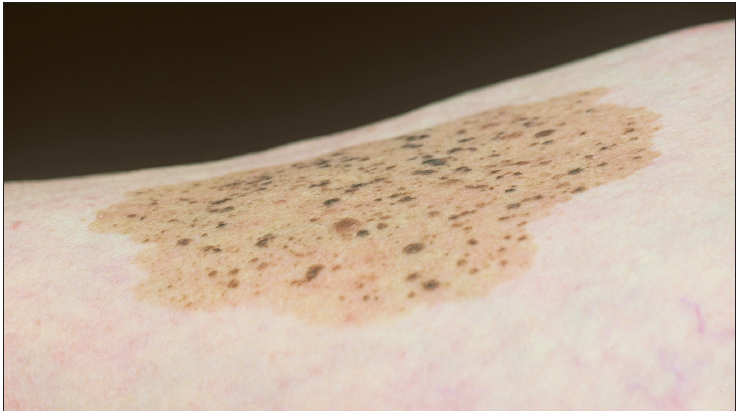
These large lesions must be followed closely over time because atypical melanocytic proliferations will lead to melanoma. Therefore, I monitor these children closely and instruct parents to contact me if the lesions change. I also recommend that congenital lesions be followed closely.
I instruct patients with "small typical lesions" that periodic assessment is approriate but I do not see these patients more often than yearly unless a change in one of the small nevi speckling the lesion suggests atypical melanocytic change. The same criteria for assessment of all pigmented lesions apply to these lesions as well (ie, ABCDE).