
Complex Regional Pain Syndrome
A 10-year-old girl presented with a 3-month history of right knee pain and difficulty walking after her pet German shepherd bumped her leg. She also complained of a 2-week history of hair growth below her right knee.
On physical examination, she had edema, a 12 × 10-cm patch of hair, and decreased range of motion of the right knee. Results of complete blood count, erythrocyte sedimentation rate, complete metabolic profile, creatine kinase tests, and myoglobin tests were normal. Findings on magnetic resonance imaging were unremarkable.

The girl received a diagnosis of complex regional pain syndrome (CRPS) and was hospitalized for inpatient physical therapy. An indwelling catheter was placed for a femoral nerve block. Ropivacaine was continued for 8 days, after which the girl was transferred to a local rehabilitation facility to continue physical therapy, along with continuous passive motion (CPM) of the knee. She was started on gabapentin, fluoxetine, vitamin D, and as-needed diazepam, and was discharged after 1 month to continue her treatment at home.
 CRPS, formerly called reflex sympathetic dystrophy, is a painful syndrome accompanied by physical changes in the affected extremity. Dysfunction of local sympathetic and autonomic nerves may be responsible.1-3
CRPS, formerly called reflex sympathetic dystrophy, is a painful syndrome accompanied by physical changes in the affected extremity. Dysfunction of local sympathetic and autonomic nerves may be responsible.1-3
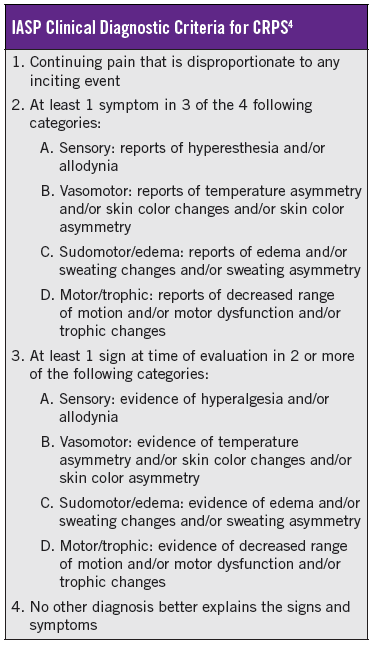
Our patient reported 3 of 4 symptoms (allodynia to clothing, edema, and decreased range of motion) and 2 of 3 signs (hyperalgesia to pinprick and allodynia to light touch) meeting the clinical diagnostic criteria for CRPS set forth by the International Association for the Study of Pain (IASP) (Table).4
The relapse rate varies from 25% to 33%, and signs and symptoms can spread from one extremity to another.5 Hypertrichosis is common in the early stages of CRPS and is thought to be the result of increased neurogenic inflammation.6
At 3 months’ follow-up, the patient had improved. She had returned to school, could ambulate without assistance, and could climb stairs but could not run. She was continuing the CPM at night, as well as the prescribed medication regimen. The hair below her right knee still was present.
References
1. Kachko L, Efrat R, Ben Ami S, Mukamel M, Katz J. Complex regional pain syndrome in children and adolescents. Pediatr Int. 2008;50(4):523-527.
2. Martin DP, Bhalla T, Rehman S, Tobias JD. Successive multisite peripheral nerve catheters for treatment of complex regional pain syndrome type I. Pediatrics. 2013;131(1):e323-e326.
3. Wilder RT. Management of pediatric patients with complex regional pain syndrome. Clin J Pain. 2006;22(5):443-448.
4. Harden RN, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150(2) 268-274.
5. Murray CS, Cohen A, Perkins T, Davidson JE, Sills JA. Morbidity in reflex sympathetic dystrophy. Arch Dis Child. 2000;82(3):231-233.
6. Nickel FT, Maihöfner C. Neuroimages: hypertrichosis in alopecia universalis and complex regional pain syndrome. Neurology. 2010;75(16):1483.