
A Collection of Fraction-Related Issues

Barton Fracture in a Soccer Player
Douglas Beall, MD, and John Whyte, MD
While playing soccer, a 24-year-old man fell on his outstretched hand, felt a “pop,” and immediately noticed a deformity of his wrist. He was in severe pain when he presented to the emergency department.
Laboratory testing. Anteroposterior and lateral radiographs of the wrist showed a distal radius fracture with dorsal dislocation of the radiocarpal joint.
Discussion. One of the most common fracture dislocations of the wrist, the Barton fracture usually extends into the wrist joint. The fracture can involve either the dorsal or volar portion of the distal radius but, by definition, has an associated dislocation of the carpus, with proximal and either dorsal or volar displacement. Often, a radial styloid fracture is also present. A Barton fracture differs from a Smith or Colles fracture because of the associated proximal carpal row dislocation. In a Barton fracture, the radial fracture fragment is generally smaller than the fracture fragments seen in Smith and Colles fractures.
Most Barton fractures are managed nonoperatively with manipulative reduction, followed by immobilization for 6 weeks. For unstable fractures, reduction with pin insertion or application of an external fixator may be necessary.
Outcome of the case. In this patient, the alignment and stability of the wrist after manipulative reduction was adequate, and a cast was placed on the wrist in extension. After 6 weeks, the cast was removed. He then underwent 6 weeks of physical rehabilitation and returned to playing soccer within 3 weeks.
Psoas Avulsion Fracture in a Baseball Player
Brady Pregerson, MD
During a baseball game, a 29-year-old man had taken a lead off first base. He then did a half pivot to rapidly plant his foot back on the base before he ran and slid into second base. Immediately after sliding into the base, he felt pain in the right groin and required assistance to walk.
He had no previous injury to the groin area. Seven years earlier, he had sustained a traumatic fracture of the ankle. He had no family history of metabolic bone or connective-tissue disorders.
Physical examination. The patient's right leg was warm, with normal reflexes and sensation, good pulses, and soft compartments. The skin was intact. Active range of motion was preserved in the knee and ankle of the right leg but was limited in the right hip, secondary to pain. He complained of pain with hip flexion and of discomfort with adduction and rotation of the right hip.
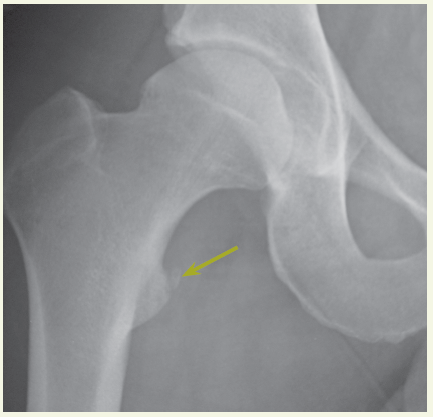
A radiograph of the pelvis showed avulsion of the lesser trochanter.
Discussion. In avulsion fractures of the pelvis, the involved muscle may be identified by the location of the fracture and, when the patient can tolerate a muscular strength evaluation, certain resistance testing clues:
• Pain with hip flexion and rotation: iliopsoas muscle has pulled off part of the lesser trochanter, as in this patient.
• Worsening pain with hip flexion and abduction: sartorius muscle has pulled off part of the anterior superior iliac spine.
• Worsening pain with hip flexion: rectus femoris muscle has pulled off part of the anterior inferior iliac spine.
• Worsening pain with hip extension: hamstring muscle has pulled off part of the ischial tuberosity.
• Pain with abduction and external rotation: piriformis muscle has pulled off part of the greater trochanter.
• Pain with adduction: hip abductor has pulled off part of the ischiopubic ramus.
Avulsion fractures of the pelvis are most common in patients between the age of 11 and 15 years. The differential diagnosis includes muscle strain and periostitis. Consider osteomyelitis or tumor in patients with groin pain who have asymmetric radiographic findings and no history of trauma.
Treatment. The healing process consists of rest and the use of crutches, with toe-touch weight bearing, for up to 2 months in most patients. A gradual return to stretching and activity is determined by the patient's symptoms; consultation with an orthopedist is recommended. Injuries with either large fragments or more than 15 mm of displacement may require surgical fixation. Complications include nonunion and healing with a bony prominence that can affect future function.
Outcome of the case. This patient was referred to an orthopedist. He fully recovered in 6 months.
Orbital Floor Fracture
Carol A. Ludin, MD, and Joel M. Schwartz, MD
Four hours before he arrived at the emergency department, a 33-year-old man had been struck in the face by a rock. A laceration and periorbital hematoma were noted on the left side of the patient’s face. He complained of pain in this area. There was no history of intraocular disease. The left globe was intact, and no neurologic deficit was found. The physician reported that a supine radiograph demonstrated interruption and widening of the floor of the left orbit.
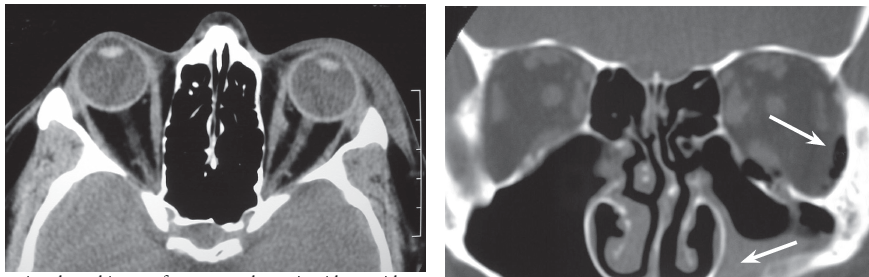
Laboratory testing. An upright radiograph revealed fluid in the left maxillary sinus consistent with hemorrhage. Orbital floor fracture was diagnosed. An axial CT scan of the orbits demonstrated widening and increased density in the periorbital fat, which indicated soft tissue swelling.

The scan was performed to evaluate the medial and lateral walls of the orbit, which were determined to be intact. A direct coronal CT scan showed the depressed fracture of the orbit floor, hemorrhagic debris in the left maxillary sinus, and intraorbital emphysema; air was noted passing through the fracture from the left maxillary sinus into the left orbit. Coronal imaging is best for visualizing the roof and floor of the orbit. If direct coronal imaging cannot be performed, thin-section axial images can be obtained with generation of coronal reformats.
Discussion. Orbital floor fractures may be caused by direct trauma to the inferior orbital rim, which results in buckling of the orbital floor. Fractures may also occur when rapidly increased intraorbital pressure is decompressed at the weakest point of the bony confines of the orbit. Suspect an orbital fracture when a patient has a history of trauma, ecchymosis with or without edema of the lids, diplopia, hypoesthesia of the cheek (related to injury to the infraorbital nerve), or emphysema of the orbit or lids. Enophthalmos and ptosis of the globe indicate a large fracture. Fractures of the orbit frequently involve the weakest part of the bony orbit—the lamina papyracea or medial wall. If the medial wall is involved, hemorrhagic debris is seen in the ethmoid complex, and air that emanates from the ethmoid results in intraorbital emphysema.
Fractures of the orbit roof and lateral wall are much less common. They can be complicated by cerebrospinal fluid leak and herniation of intracranial contents into the orbit; entrapment of the superior rectus muscle is rare.
Treatment. Most orbital floor fractures heal without treatment, as in this case. Consider surgical repair in the event of complications, such as sensory disturbance as a result of injury of the infraorbital nerve, muscle entrapment when the inferior rectus herniates through the fracture defect, and enophthalmos from herniation of large portions of orbit contents into an adjacent sinus.
Fracture of the Scapula
Luis Cabrera, MD, Ali Ahmadizadeh, MD, and John Carmody, MD
A 56-year-old man, who was involved in an automobile accident, was brought to the emergency department by ambulance. He was awake, intoxicated with alcohol, and complained particularly of pain in his left shoulder. The patient was unable to recall any details of the accident; he believed that he had been hospitalized for a back spasm. Because of the patient’s discomfort, physical examination of his left shoulder was limited.
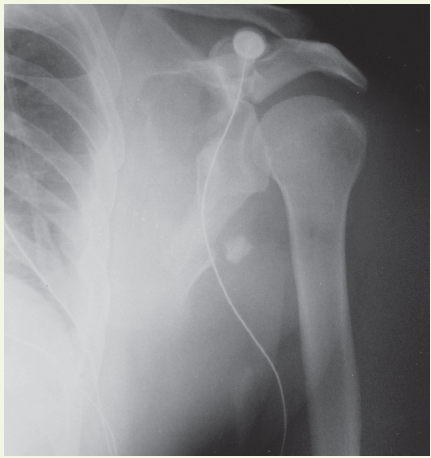
Laboratory testing. Muscular or ligamentous injury was initially suspected, and a roentgenogram of the shoulder was obtained. The film revealed a comminuted fracture of the left scapula that involved the neck, body, and spine. The glenohumeral relationship was maintained. Also visualized was a fracture of the posterolateral aspect of the fourth through eighth ribs, an injury which can increase the risk of a tension pneumothorax, hemothorax, or pulmonary and visceral injury.
Discussion. The physician noted that a scapular fracture may occur from direct violence, sudden contraction of divergent muscles, or electric shock. Fractures to the body of the scapula, which usually result from high-energy trauma, are associated with the greatest morbidity. A plain x-ray film is diagnostic; a CT scan can detect involvement of the glenoid fossa.
Treatment. Because of the potential life-threatening complications that may occur in this setting, this patient was admitted to the ICU; he was immobilized, ice was applied locally, the rib fracture was managed conservatively, and analgesics were given. Healing may take between 4 and 6 weeks, depending on the patient’s general condition.
Reduction of the scapula usually is not required, unless the fracture involves major displacement of the glenoid fossa.
Pathologic Femur Fracture
Wael AlJaroudi, MD, MS
 A 41-year-old woman presented to the emergency department (ED) with a 3-day history of left thigh pain and swelling. She denied any precipitating trauma. The symptoms started after she woke up and found her boyfriend’s leg lying over her thigh. Because of the severity of the pain, she was unable to walk.
A 41-year-old woman presented to the emergency department (ED) with a 3-day history of left thigh pain and swelling. She denied any precipitating trauma. The symptoms started after she woke up and found her boyfriend’s leg lying over her thigh. Because of the severity of the pain, she was unable to walk.
She reported a 25-lb weight loss during the past year and a chronic nonproductive cough, but no shortness of breath, hemoptysis, fever, or history of travel. She smoked cigarettes and cocaine, and she had a history of chronic alcoholism. The patient also had chronic hepatitis C and alcoholic liver cirrhosis with portal hypertensive gastropathy but no esophageal varices. An ultrasound examination of the liver several years earlier had shown multiple hypoechoic lesions, which could be regenerating nodules, but hepatocellular carcinoma could not be excluded. A CT scan of the abdomen was recommended, but the patient was lost to follow-up until her recent presentation to the ED.
Physical examination. Her temperature was 37.4°C (99.3°F); blood pressure, 114/58 mm Hg; pulse, 120 beats per minute; and respiration rate, 16 breaths per minute. Oxygen saturation was 94% on room air. She weighed 45 kg (99 lb) and appeared cachectic.
Neck was supple with no thyroid enlargement, and no lymph nodes were palpable. Breast examination revealed no masses. Breath sounds were decreased in the right lower base. The edge of the liver was palpable, but there was no ascites or splenomegaly. Swelling and tenderness were noted in the distal thigh. Rectal examination was unrevealing, and the stool guaiac test was negative.
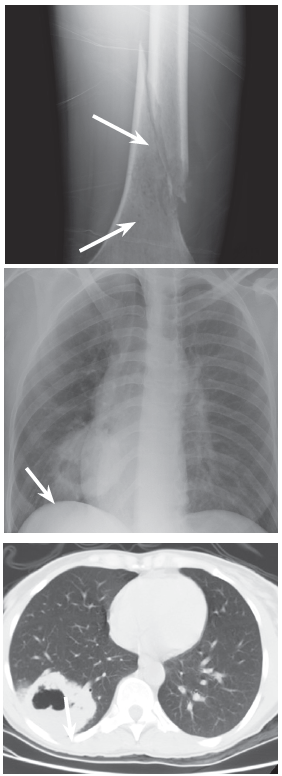
Laboratory testing. A radiograph of the femur showed an aggressive mottled lesion in the distal diaphysis with a pathologic fracture. A chest radiograph revealed a 6-cm round mass in the right lower lung with central lucency, clearly defined by a chest CTscan as a thick-walled cavitary mass.
Results of a GI panel; calcium, phosphorus, alkaline phosphatase, and alpha-fetoprotein levels; and serum protein electrophoresis (SPEP), urine protein electrophoresis (UPEP), and urinalysis results were normal. Acid-fast bacillus and fungal sputum cultures were negative. White blood cell count was 12,000/µL, and erythrocyte sedimentation rate (ESR) was 42 mm/h. A bone scan showed increased uptake in the distal femur only. CT scans of the brain, abdomen, and pelvis were negative.
The patient’s thigh was splint, and she was admitted to the hospital. She then underwent repair of the fracture; intra-operative femur tissue biopsy showed metastatic poorly differentiated non-small cell carcinoma. Immunoperoxidase staining suggested primary lung adenocarcinoma. The patient received 800-centigray radiation palliative therapy to the left femur and was scheduled for outpatient palliative chemotherapy.
Discussion. A pathologic fracture occurs in abnormal bone, typically with normal activity or minimal trauma.1 Common causes are osteoporosis, osteomalacia, Paget disease, osteopetrosis, osteogenesis imperfecta, fibrous dysplasia, primary benign tumor, primary malignant tumor, and metastatic tumor. Relevant history includes degree of trauma, constitutional symptoms, previous history of malignancy, smoking, dietary habits, and exposures. A stool guaiac test and palpation for lymphadenopathy, thyroid nodules, breast masses, prostate nodules, and rectal masses are warranted.
Radiographs should be carefully assessed for osteopenia, periostal thickening, abnormal radiodensities, and calcifications of small vessels. Malignant and metastatic lesions are usually eccentric and involve the cortex. New bone formation suggests osteosarcoma; calcifications are seen in chondrosarcomas; and periostal thickening is less likely to be malignant. If a suspected metastatic lesion is found, a full skeletal survey should be done; common sites of bone metastasis include the spine, ribs, pelvis, femur, and humerus. If a bone scan shows uptake at 5 or more sites, metastatic malignancy is almost certain. Commonly indicated laboratory studies include a complete blood cell count, urinalysis, SPEP, UPEP, liver function tests, and measurement of alkaline phosphatase, calcium, phosphorus, ESR, and prostate-specific antigen in males.
Treatment. Diagnosis is made by CT-guided core biopsy or open biopsy. Treatment includes radiation, chemotherapy, pain management, and surgical fixation if there is persistent pain after irradiation, destruction of the bone, and interference with activity.
REFERENCE:
1. Dick HM, Rosenberg AE. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 26-1995. A previously well, 29-year-old woman with a pathologic fracture of the femur. NEJM.1995;333(8):507-511