
Children With the Same Congenital Malformation Pattern

Figures A-D show 4 children with the same congenital malformation pattern. Children with this disorder often have a low birth weight and feeding problems in the nursery, with severe gastroesophageal reflux. Their cry is frequently low-pitched and growling. Among the characteristic birth defects are those that affect the limbs, as shown in these patients.

WHAT IS THE DIAGNOSIS—AND WHAT MEDICAL COMPLICATIONS CAN BE EXPECTED?
WHAT ANOMALIES MAKE THE FACIAL APPEARANCE CHARACTERISTIC?
ANSWERS:
- Brachmann-de Lange syndrome. Affected children have mental disability and behavior and GI defects.
- The minor anomalies that produce the rather grim and characteristic facial appearance include low frontal hairline (Figure D), thick and arched eyebrows, joining of the eyebrows at the midline (synophrys), upturned nose (anteverted nares), down-turned corners of the mouth, long philtrum, and thin upper lip.
APPROACH TO DIAGNOSIS
Humans have a remarkable ability to recognize and remember faces, a skill essential for maternalinfant bonding. Neurons that promote the skill are situated in the pons; their power is emphasized after injury when a person loses the capacity to recognize faces (prosopagnosia). Developmental disorders often affect the face, producing a characteristic appearance that allows the experienced physician to make a snap diagnosis. This “gestalt” impression can be buttressed by an analysis of the facial anomalies so that there is less chance of being misled by hasty judgments or familial resemblance. Most important for the primary physician is to recognize an unusual appearance (the term “funny-looking kid” has been discarded for obvious reasons). This will fuel suspicion of a syndrome and allow for early referral, genetic counseling, and preventive health care. Although syndrome identification can be attempted by thumbing through the classic and now colorful reference by Jones,1 recognition of a possible syndrome is the important step.
A textbook by Gorlin and colleagues2 and, for mendelian syndromes, the database Online Mendelian Inheritance in Man3 can be consulted for more details, references, and availability of DNA testing for specific syndrome disorders. The database is available at OMIM and at www.ncbi.nlm.nih.gov/sites/entrez? db=omim (Enter Brachmann or Cornelia de-Lange). All of these references describe the Brachmann-de Lange syndrome (BDLS)—a disorder so characteristic that syndrome pioneer John Opitz recognized the earlier discovery of W. Brachmann when salvaging library books damaged by a burst pipe: “In the fall of 1963 . . . [I was asked to look at] Jahrbuch fur Kinderheilkunde . . . volume 84, dated 1916, the pages of which were completely glued together except for one place, the article beginning on page 225 . . . here was an article on the Cornelia de Lange syndrome written 17 years before de Lange’s first paper of 1933. The author, Dr W. Brachmann, whose subsequent fate is unknown to me, was then a young physician in training, who apologized that his study of this remarkable case was interrupted by sudden orders to report for active duty (in the German Army).”4 Dr Opitz thus re-stored Brachmann’s name to the disorder and contributed much to its delineation.
CLINICAL FINDINGS
BDLS has a birth incidence of at least 1 in 10,000. This is perhaps an underestimation because of early deaths from feeding or infectious problems. The facial appearance is distinctive and usually evident at birth, although some patients may present because of early growth delay.5,6 Low frontal hairline, heavy and arched eyebrows joined in the midline, thin upper lip, long philtrum, and down-turned corners of the mouth produce a grim facial appearance that is unforgettable. A low-pitched and growling cry and a grayish hue to the face enhances the grim appearance. Infants with BDLS are stiff and hypertonic, with vascular changes that can produce perioral cyanosis in the absence of cardiorespiratory disease.
The most striking associated anomalies (Table) are limb deficiencies that range from oligodactyly (Figure A) to peromelia (tapered distal limbs—Figure D) or phocomelia (flipper limbs).5,6 Other limb anomalies include small hands and feet, proximally placed thumbs, fifth finger clinodactyly, or syndactyly of toes 2 and 3.
The head is small with a flat occiput (microbrachycephaly). The IQ for severely affected children ranges from 30 to 86, with an average of 53.1 Children with less striking findings and/or with affected relatives will have a better cognitive prognosis. Sensorineural or conductive hearing loss from early otitis may contribute to speech delay, and vision may be affected by myopia, strabismus, or early glaucoma with globe enlargement (buphthalmos). Behavior differences can include antiso cial and autistic manifestations with repetitive and selfdestructive movements.
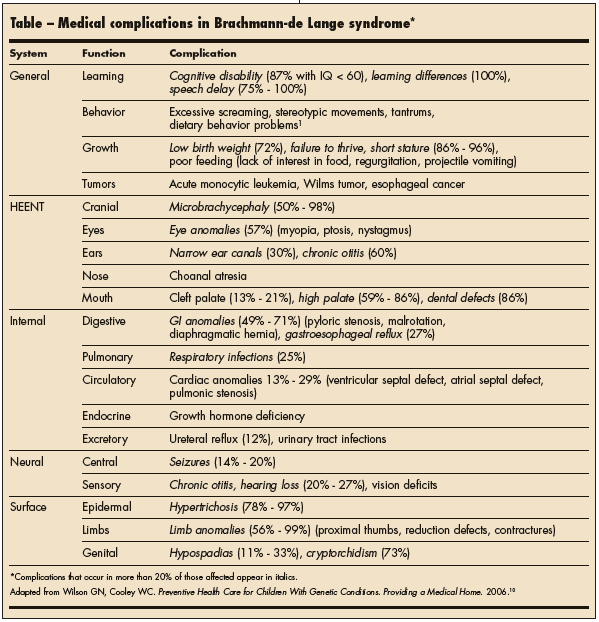
Internal anomalies, such as malrotation, volvulus, and pyloric stenosis, often lead to GI problems, such as dysphagia, gastroesophageal reflux, projectile vomiting, or failure to thrive. Cardiac defects may augment a predisposition to respiratory infections, and genital anomalies can include hypospadias, cryptorchidism, or bicornuate uterus. Risk of malignancy, particularly adenocarcinoma of the esophagus, may be increased.
DIAGNOSTIC EVALUATION AND GENETIC COUNSELING
Chromosome studies are indicated for any child with multiple anomalies and/or unexplained developmental delay, including children with suspected BDLS. Findings from chromosome studies will be normal unless the child has dup(3q) syndrome (duplication of the long arm of chromosome 3)—a condition that manifests with a facial appearance similar to that of BDLS but is associated with more frequent internal anomalies.5-7
Severe BDLS is caused by new gene mutations; some with milder cases exhibit autosomal dominant or X-linked recessive inheritance. Referral of rare, multigeneration BDLS families by alert practitioners led to pinpointing of mutations in a Nipped-B gene that had been identified as a developmental regulator in the fruit fly.8 Roughly half of BDLS patients will have mutations in Nipped-B or other genes, allowing DNA (gene) testing that is still specialized and expensive.3,9
Thus, BDLS diagnosis remains clinical. It is assumed that most cases result from new mutations; the 2% to 5% recurrence risk cited for future pregnancies acknowledges rare inheritance or germline mosaicism. Developments in rapid sequencing and array analysis (DNA chips) may soon provide sensitive prenatal and postnatal diagnosis of BDLS.
CLINICAL COURSE AND MEDICAL MANAGEMENT
Some 5% of children with BDLS have early deaths from apnea, aspiration, cardiac anomalies, or postoperative events. Cleft or high-arched palate and narrow external auditory canals often lead to chronic otitis, which increases the chances for hearing loss. Ophthalmological problems can include ptosis that necessitates chinlifting to achieve vision. Communication may be impaired by visual or hearing problems and behavior differences: only 4% of children had low-normal to normal speech by age 4.5,6
Management of infants with BDLS includes attention to early feeding and screening for cardiac and urinary tract anomalies in the nursery.10 Early intervention services and monitoring of growth, hearing, and vision are important in early childhood. Later preventive measures may include frequent urinalyses (to rule out urinary tract infection), dental care (for the detection and correction of tooth anomalies), and physical/occupational therapy (to minimize the effects of contractures and hip malpositioning).
School performance should be monitored based on the risks of behavioral or cognitive dysfunction. Growth hormone deficiency has been reported, and growth hormone therapy may be considered for patients with higher function. Management should include planning for medical and financial services appropriate for children with significant developmental disability.5,6,10