
Can You Identify These Sun-Induced Lesions? Part 2
Photo Quiz
Case 1: Erythematous Lesion
This asymptomatic lesion has been present on the upper lip of a 41-year-old man for over a year. He works outdoors and has had extensive sun exposure.

Would you biopsy this lesion?
(Answer on next page)

ANSWER—Case 1: Basal cell carcinoma
This basal cell carcinoma (BCC) was excised along with surrounding tissue. Solar keratoses and chronic inflammation also were present on microscopic examination.
BCC is not only the most common skin cancer, it is the most prevalent form of cancer in the United States. BCCs are induced by UV-B exposure and may occur at sites of previous trauma, such as scars and burns. They are most common in persons older than 40 years. Sun exposure and fair skin are the primary risk factors; the risk rises as the amount and duration of exposure to UV radiation—particularly UV-B rays—increases. Most BCCs occur on the head and neck.
Nodular BCC is the most common form; it presents as a pearly white or pink nodule. As the nodular lesion grows, a slightly elevated rim with a flattened smooth or ulcerated center can form.
The goal of treatment is the complete removal or destruction of the lesion with the best cosmetic result. BCCs can almost always be treated in an office setting. Options include surgical excision, electrodessication and curettage, cryosurgery, Mohs micrographic surgery, and radiation.
Prevention is the key aspect of the treatment of BCCs. Emphasize to patients the importance of avoiding sun exposure, and advise them to use sunscreen daily. ■
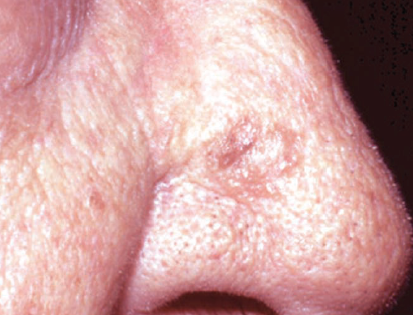
Case 2: Raised Lesion
During a routine physical examination, this raised, pink lesion is noted on an 84-year-old man’s nose. The patient reports that the lesion has been present for at least several months. It is asymptomatic.
What are you looking at here?
(Answer on next page)
ANSWER—Case 2: Actinic keratosis
The lesion was removed by excision. Histopathologic examination of an excised specimen revealed actinic keratosis and marked solar elastosis of the dermis with minimal atypia.
Actinic keratosis is confined to the epidermis. It typically occurs on sun-exposed areas; the incidence increases with age. An untreated lesion may involve deeper skin layers and develop into full-fledged squamous cell carcinoma. To assuage fears about cancer, stress to patients that actinic keratosis is premalignant, but advise them to monitor their skin for possible recurrence.
Actinic keratoses may be solitary, or several may occur on sun-exposed areas. Inflammation, induration, and oozing herald the development of a true malignancy. Clinical variants include cutaneous horns, pigmented actinic keratoses, and actinic cheilitis. Biopsy—incisional or excisional, depending on the size of the lesion—is necessary for diagnosis.
Treatment modalities include surgical removal, cryotherapy, and topical 5-fluorouracil and imiquimod creams or diclofenac gel. Advise patients with actinic keratoses to use sunscreen daily. ■