
Boy With Fever, Abdominal Pain, and Diarrhea
A 4-year-old boy is admitted with a 2-week history of high fever with rigors; profuse night sweats; progressive dull, aching, nonradiating right upper quadrant pain; and watery, foul-smelling diarrhea that contains no blood or mucus.
 History. The child has stable bronchial asthma; his history is otherwise unremarkable. His milestones have been within the normal range. He has no allergies and has not traveled outside the country; his immunizations are up to date.
History. The child has stable bronchial asthma; his history is otherwise unremarkable. His milestones have been within the normal range. He has no allergies and has not traveled outside the country; his immunizations are up to date.
His temperature has been consistently high for the past 72 hours. He has lost about 10 lb during the past month. His appetite is poor. He has a dry, irritating cough, but no chest pain, dyspnea, palpitations, ankle edema, nausea, vomiting, melena, hematemesis, or jaundice. He has no history of headache, vision problems, neck stiffness, weakness, seizures, syncope, urinary symptoms, or rash. He has not been in contact with ill persons. The family history is noncontributory.
Examination. The patient appears ill, thin, and poorly nourished. He cries easily, but his mother is able to console him. His heart rate is 120 beats per minute and regular; temperature, 38.8°C (102°F); respiration rate, 20 breaths per minute; blood pressure, 98/63 mm Hg. Hydration status is good. Examination of the head and neck reveals generalized pallor but no icterus or candidal infection. There is no palpable adenopathy. Abdominal examination reveals upper abdominal distention; a smooth, tender, liver enlarged to 5 finger breadths; and intercostal tenderness. There is no splenomegaly or ascites. Jugular vein pulse and heart sounds are normal. The lungs are clear to auscultation and percussion. The results of a neurologic examination are normal; there are no meningeal signs and there is no neck stiffness.
Laboratory studies. Hemoglobin level, 10.6 g/dL; hematocrit, 33.3%. White blood cell (WBC) count, 17,200/μL, with 58% polymorphonuclear leukocytes, 16% bands, 25% lymphocytes, and 1% eosinophils. Platelet count, 325,000/μL; erythrocyte sedimentation rate (ESR), 110 mm/h. Results of urinalysis, normal. Blood urea nitrogen level, 15 mg/dL; creatinine, 0.8 mg/dL; serum sodium, 135 mEq/L; potassium, 4.4 mEq/L; chloride, 90 mEq/L. Blood glucose, 90 mg/dL; total bilirubin, 1.8 mg/dL; conjugated bilirubin, 1.2 mg/dL. Alkaline phosphatase, 200 U/L. Total protein, 5.7 g/dL; albumin, 1.7 g/dL; aspartate aminotransferase, 75 U/L; alanine aminotransferase, 68 U/L. Stool cultures are negative for organisms. Clostridium difficile toxin test results are negative. Ova and parasite examination reveals Giardia cysts.
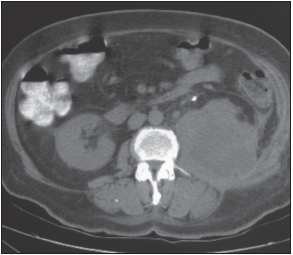
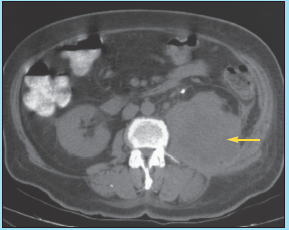
An ultrasonogram of the abdomen discloses a large hypodensity in the right lobe of the liver. The abdominal CT scan is shown here.
In view of the clinical picture and the abnormalities evident on the imaging studies, what is the most likely diagnosis?
A. Amebic liver abscess
B. Pyogenic liver abscess
C. Hydatid cyst
D. Necrotizing hepatoma
E. Cavernous hemangioma
Answer on next page
WHAT’S WRONG:
The abdominal CT scan shows a large, welldemarcated, hypodense lesion in the right lobe of the liver, consistent with an abscess. Features that strongly suggest pyogenic liver abscess, B, include high fever, progressive upper right quadrant pain, an enlarged liver, and a large hypoechoic lesion on ultrasonograms and CT scans.
Hospital course. The patient is hospitalized for further evaluation. Additional laboratory results include hemagglutination titers negative for amebae and 4 negative blood cultures. CD4+ cell count, 1221/μL. Immunoglobulins: IgA, 247 mg/dL (normal, 33 to 235 mg/dL); IgG, 1172 mg/dL (normal, 592 to 1723); IgM, 97 mg/dL (normal, 36 to 314 mg/dL); IgE, 66 U/mL (normal, less than 61 U/mL). Complement: CH50, 46 U/mL (normal, 31 to 66 U/mL).
 Aspiration of the abscess produces purulent, foulsmelling fluid. Gram staining of a fluid sample reveals a red blood cell count of 10,000/μL; WBC count, 950,000/μL, with 97% neutrophils; and Gram-positive and Gram-negative cocci and bacilli. Culture of the fluid grows aerobes (Escherichia coli and Klebsiella pneumoniae) and anaerobes (Peptococcus, Bacteroides fragilis, and Prevotella). The growth of Gram-negative and anaerobic pathogens from the fluid confirms the diagnosis of pyogenic liver abscess.
Aspiration of the abscess produces purulent, foulsmelling fluid. Gram staining of a fluid sample reveals a red blood cell count of 10,000/μL; WBC count, 950,000/μL, with 97% neutrophils; and Gram-positive and Gram-negative cocci and bacilli. Culture of the fluid grows aerobes (Escherichia coli and Klebsiella pneumoniae) and anaerobes (Peptococcus, Bacteroides fragilis, and Prevotella). The growth of Gram-negative and anaerobic pathogens from the fluid confirms the diagnosis of pyogenic liver abscess.
Results of a hepatitis panel, serologic test for cocci, and tuberculosis skin test are all negative. A chest radiograph shows no infiltrates.
The patient is initially treated with IV metronidazole, 200 mg every 8 hours. After aspiration, piperacillin with tazobactam, 1.5 g every 8 hours, is added. Percutaneous catheter drainage is established. After a week, the drainage fluid is less than 10 mL in 24 hours. A repeated abdominal CT scan reveals almost complete resolution of the abscess, and the drain is removed. The symptoms, including fever and pain, resolve within a week.
The patient will continue to receive intravenous antibiotics for 2 more weeks. Acute surgical intervention is deemed unnecessary because of the patient’s improvement. The abdominal CT scan will be repeated in a month. If it shows a fecalith in the appendix, the appendix may be removed on an elective basis.
OVERVIEW
Liver abscesses are caused by bacterial, parasitic, or fungal infections. Pyogenic abscess accounts for three quarters of hepatic abscesses in developed countries. Elsewhere, amebic abscesses are more common.
Bacterial abscess of the liver is relatively rare in children and may present diagnostic and therapeutic challenges.
EPIDEMIOLOGY
The incidence of pyogenic liver abscess in the United States is estimated to be 8 to 15 cases per 100,000 population; the autopsy rate ranges from 0.29% to 1.47%. The male-to-female ratio is approximately 2:1. The condition occurs most commonly in the fourth to sixth decade of life.
Liver abscesses in infants are associated with umbilical vein catheterization and sepsis. Liver abscesses in children frequently involve immunodeficiency or trauma.
ETIOLOGY
Pyogenic bacteria may gain access to the liver by direct extension from contiguous organs or through the portal vein or hepatic artery. Hepatic clearance of bacteria via the portal system is normal in healthy persons; however, organism proliferation, tissue invasion, and abscess formation may occur with biliary obstruction, poor perfusion, or microembolization.
Infection via the portal system (portal pyemia) originates within the abdomen and reaches the liver by embolization or seeding of the portal vein. Appendicitis is the predominant cause in children; other causes include inflammatory bowel disease, diverticulitis, and proctitis.
Biliary disease accounts for 21% to 30% of cases of pyogenic liver abscess in adults with stones, strictures, or malignancy. Hematogenous spread via the hepatic artery can occur with systemic bacteremia, as in the setting of endocarditis.
No cause is found in approximately half of cases.
MICROBIOLOGY
Most patients with pyogenic liver abscess have a polymicrobial infection of biliary or enteric origin. Blood cultures are positive in 33% to 65% of cases; abscess cultures are positive in 73% to 100% of cases.
The most common microorganisms isolated from blood and abscess cultures are Streptococcus species (37%), E coli (33%), K pneumoniae (18%), Bacteroides species (24%), microaerophilic streptococci (12%), and Staphylococcus aureus.
CLINICAL FEATURES
The classic presentation consists of right upper quadrant pain (89% to 100% of patients) and fever (87% to 100%) associated with chills, anorexia, and malaise (38% to 80%), and weight loss (25% to 68%). Fever of unknown origin is frequently the initial diagnosis in indolent cases.
Clinical findings are most notable for right upper quadrant tenderness (41% to 72%), hepatomegaly or liver mass (51% to 92%) and, less commonly, jaundice (23% to 40% of cases in later stages). Decreased breath sounds in the right basilar area, with signs of atelectasis and effusion, are occasionally present.
DIAGNOSIS
A diagnosis of pyogenic liver abscess is usually established by:
•Positive blood cultures.
•Radiologic evaluation, including:
—A CT scan, which shows the size and location of the abscess or abscesses and the number of abscesses.
—An ultrasonogram, which indicates a rounded or hypoechoic mass (80% to 100% sensitivity).
—A radionucleotide sulfur colloid scan, which can detect abscesses larger than 2 cm.
—A plain abdominal radiograph, which may show hepatomegaly, sometimes with an air-fluid level in the abscess cavity. The right diaphragm is often raised, with pleural reaction or pneumonic consolidation.
•CT-guided diagnostic aspiration. Culture and Gram staining help identify the offending pathogens.
Two thirds of patients have appreciable leukocytosis, often accompanied by anemia of chronic infection and an elevated ESR. Results of liver function tests are usually normal.
TREATMENT
Management involves antibiotic therapy and drainage of the abscess, either percutaneously or surgically.
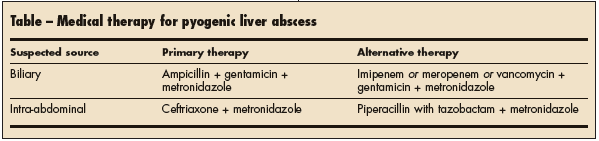
Empiric broad-spectrum parenteral antibiotic treatment must be started as soon as an abscess is diagnosed. Select antimicrobial agents that provide adequate coverage against aerobic Gram-negative bacilli; microaerophilic streptococci; and anaerobic organisms, including B fragilis. Usually, a combination of 2 or more agents is used (Table).
Specific antibiotic therapy is tailored once microbiologic data and sensitivity results are available. Treatment is continued for 2 to 4 weeks, depending on the number of abscesses, the underlying pathogens, and the clinical response.
Percutaneous catheter drainage under ultrasonographic or CT guidance permits recovery of diagnostic material and removal of pus to hasten recovery. Drainage is continued until a CT scan documents collapse of the cavity. Open surgical drainage is performed when:
•An abscess is not amenable to percutaneous drainage because of location.
•Comorbid intra-abdominal disease requires surgery.
•Antibiotic therapy with percutaneous drainage is unsuccessful.