
Biological and Pharmacological Treatment of Post-traumatic Stress Disorder in Older Adults
Affiliations:
1Department of Psychiatry and Behavioral Medicine, University of South Florida, Tampa, FL
2Department of Medical Education, University of Central Florida, Orlando, FL
Abstract: This article focuses on the current state of treatment for post-traumatic stress disorder (PTSD), with an emphasis on meeting the needs of older adults and elderly persons who are in the early stages of PTSD or who have chronic PTSD. The authors review some of the pre-disaster and post-disaster interventions that clinicians can employ if older patients present with early signs and symptoms of PTSD. The authors discuss how concepts such as disaster immunization, resilience, and psychological first aid affect treatment of PTSD. In some patients, use of medication to treat the symptoms of PTSD may be necessary. This article gives an overview of the considerations and evidence to guide safe and appropriate prescribing of a pharmacologic agent—namely antidepressants and benzodiazepines—to treat the symptoms of PTSD. The final article in the series will discuss psychotherapeutic approaches to treat PTSD.
Article series summary: This is the third article in a continuing series on post-traumatic stress disorder (PTSD). The first article in the series, “Post-Traumatic Stress Disorder: A Historical Perspective of an Evolving Diagnosis” was published in the June issue online, and the second article in the series, “Prevention and Screening of Post-Traumatic Stress Disorder in Older Adults,” was published in the July issue online. The final article, which will be published online in September, will discuss the psychotherapeutic approaches to treatment of PTSD in older adults.
Key words: Post-traumatic stress disorder, psychological first aid, disaster immunization, disaster inoculation, acute stage of trauma.
________________________________________________________________________________________________________________________________
Since post-traumatic stress disorder (PTSD) was officially recognized as a diagnostic entity in the Diagnostic and Statistical Manual-III (DSM) in 1980,1 there has been research on the underlying neurobiological changes that occur in PTSD and the efficacy of a myriad of treatments options. Much of this research has been directed to the study of young and middle-aged adults, particularly veterans, rape victims, and survivors of catastrophic disasters.1-7 Many of these studies, for practical reasons, took place in the Veterans Administration (VA) system, rape treatment centers, and/or specialty university clinics, where the elderly were usually an underrepresented group.1-3,7 Such research has, at times, been criticized for its inconsistent definition and the unreliability of the symptoms measured due to evolving diagnostic standards8; the large number of comorbid conditions, such as substance abuse and personality disorder, in persons with PTSD; and the frequent invocation of the condition in litigation (eg, disability claims).2,3,7
Historically, the elderly population has rarely been considered to be the focus of a primary study group, since it was believed that their likelihood of exposure to traumatic events was infrequent. For example, older persons were not considered to be in situations where physical violence or trauma would occur, such as fighting in wars, working in dangerous jobs (eg, police officers), or participating in crowded social events.1,4-6 When elderly individuals were included in clinical studies, they were often a subset of a large cohort study, most often one focusing on the general prevalence of symptoms occurring following a disaster, but the study did not specifically examine their response to treatment.5
This article, the third article in a continuing series on PTSD in older adults, focuses on the current state of treatment for PTSD in these individuals. In the next and final article of the series, which will be published in next month’s issue, we will discuss common psychotherapeutic approaches to PTSD, including cognitive behavioral therapy, prolonged exposure therapy, psychodynamic psychotherapy, and eye movement desensitization reprocessing treatment. While reading through this discussion, it is important for clinicians to note the limitations of the literature and to try to determine its applicability to the diagnosis and treatment of their geriatric patients.
Treating PTSD With Pre-disaster and Post-disaster Interventions
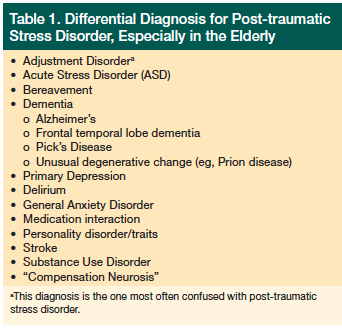 Before treating PTSD, healthcare providers should rule out other diagnoses (Table 1). When treating victims immediately following a traumatic event, public health officials have put forward the concepts of disaster immunization, disaster inoculation, and psychological first aid.9 Disaster immunization refers to the notion that pre-disaster interventions can reduce or diminish the likelihood that individuals will develop psychiatric conditions following the disaster.9 The concept of disaster inoculation involves the engagement of groups of individuals who have already been exposed to trauma or who are going to be imminently exposed and maintaining their functionality by reducing short-term and long-term sequela from stress.9-11 It is no coincidence that the terms inoculation and immunization, which are commonly used in virology, are applied in the clinical care of PTSD. Many public health officials and disaster planners view “containing” panic after a disaster and providing “herd immunity” as a primary means of maintaining order and public function in the short term, and preventing large-scale pandemics of psychiatric and stress-related physical symptoms in the long term.9
Before treating PTSD, healthcare providers should rule out other diagnoses (Table 1). When treating victims immediately following a traumatic event, public health officials have put forward the concepts of disaster immunization, disaster inoculation, and psychological first aid.9 Disaster immunization refers to the notion that pre-disaster interventions can reduce or diminish the likelihood that individuals will develop psychiatric conditions following the disaster.9 The concept of disaster inoculation involves the engagement of groups of individuals who have already been exposed to trauma or who are going to be imminently exposed and maintaining their functionality by reducing short-term and long-term sequela from stress.9-11 It is no coincidence that the terms inoculation and immunization, which are commonly used in virology, are applied in the clinical care of PTSD. Many public health officials and disaster planners view “containing” panic after a disaster and providing “herd immunity” as a primary means of maintaining order and public function in the short term, and preventing large-scale pandemics of psychiatric and stress-related physical symptoms in the long term.9
One form of inoculation treatment is referred to as psychological first aid.12 The primary goals of psychological first aid are to provide symptomatic relief (eg, reduce anxiety, facilitate sleep, ensure safety) and reassurance, and to mobilize the patient’s support networks, resources, and coping skills.12 It is not the goal of psychological first aid to provide therapy in the immediate aftermath of a crisis, but rather to stabilize, triage, and refer. Psychological first aid and other inoculation interventions are not intended to be forms of psychological debriefing, a term that traditionally describes varying forms of either group or individual counseling where aspects of the event are discussed within close proximity of the traumatic event. Debriefing, with even a single-session of “counseling” immediately after experiencing a trauma, is not advised because many studies have shown this approach has the potential to cause harm.13-17 For example, a literature review by Aulagnier and colleagues revealed that psychological debriefing often results in re-exposure to the traumatic event, which can interfere with the natural course of adjustment and recovery, potentially leading to worse outcomes even after just one session.16
When individuals are in an acute hyperarousal state immediately following a trauma, it is considered poor care to force mental processing or further recounting of the event since these interventions have been shown to increase fear, helplessness, shame, vulnerability, and a sense of lack of control.1,12,16
With regard to elderly persons, the closest clinical concept to immunization is that of resiliency. The literature reveals a divided opinion concerning whether the elderly are more or less resilient to the effects of trauma.5 Studies suggests that patients most likely to develop PTSD after a single large-scale event are individuals in their 20s to 30s, with those older than 65 years being least likely to demonstrate symptoms of PTSD.5 It is unclear why this is the case, but numerous reasons have been suggested. Some investigators have speculated that people develop better coping skills as they age, whereas others suggest that vulnerable individuals with predisposition for developing PTSD (eg, substance abuse, personality disorders) do not live as long, and yet others think that elderly individuals have more intact social support networks and resources than younger patients.5,18 On the other hand, some studies indicate that elderly persons are not more resilient than other age groups; for example, trauma studies frequently underreport the true number of affected elderly persons because of differences in the symptomatic presentation of older adults compared with younger adults; isolation and poverty are two potential risk factors for PTSD that can affect elderly and young alike.5,18,19
Treatment During the Acute Stage of Trauma in the Outpatient Primary Care Setting
Many studies on symptom development following trauma show that psychiatric symptoms are not the most prevalent immediately following the event, but that they occur or are at least first identified 3 to 6 weeks after the event.4,5,20,21 One of the key features of PTSD is avoidance, which often results in individuals being reluctant to seek help for their symptoms because they do not want to discuss the event.3 The avoidance and potential anticipatory anxiety that these patients feel when they think about or discuss the event may cause them to isolate themselves from friends and family, drop out of treatment, or be unwilling to participate in certain forms of treatment, such as exposure-based therapies. Many older persons with low mood or heightened anxiety do not volunteer information about symptoms of emotional or psychological distress to their healthcare provider, but instead present with vague or nonspecific somatic problems.18 They tend to normalize their feelings with statements such as, “Everyone feels a little anxious or blue some days,” or make statements such as, “I don’t want to be a bother/burden,” or “I have no energy and my arthritis pain is worse.” These patients usually see their primary care physicians for physical issues before they or their family realizes that the primary problem is psychiatric.
 People exposed to a trauma frequently question how they feel, what they should feel, or if their feelings or experiences are normal or abnormal.1,12 It is important for healthcare providers, as well as patients, to realize that not every psychological response is pathological (Table 2).22 Having an understanding of what constitutes a “normal” reaction to an abnormal situation and the expected timeframe for symptom resolution (peaks within days to weeks with full resolution over the course of 1 to 3 months) may reduce anxiety and the overall likelihood of developing a more persistent condition.1,12 A helpful intervention at this stage is to reassure the patient that his or her response is common, is not necessarily pathological, and that most people soon overcome their fear and return to a normal pre-trauma level of functioning. The physician’s goals should include reinforcing the patient’s strengths, encouraging use of existing support networks, offering referral for counseling if it is needed (eg, for more persistent and significant symptoms that impair function), offering a follow-up appointment within 2 to 4 weeks to monitor symptom progression and severity, and educating the patient to look for warning signs of a greater problem that will require a more immediate intervention (eg, suicidal ideation, significant impairment in functioning, or symptoms that do not improve or worsen over an additional 2 to 3 weeks). In general, the sooner the individual is able to return to his or her normal level of functioning and routine, the less likely it is that he or she will develop chronic, debilitating symptoms of PTSD.1,12,20,21
People exposed to a trauma frequently question how they feel, what they should feel, or if their feelings or experiences are normal or abnormal.1,12 It is important for healthcare providers, as well as patients, to realize that not every psychological response is pathological (Table 2).22 Having an understanding of what constitutes a “normal” reaction to an abnormal situation and the expected timeframe for symptom resolution (peaks within days to weeks with full resolution over the course of 1 to 3 months) may reduce anxiety and the overall likelihood of developing a more persistent condition.1,12 A helpful intervention at this stage is to reassure the patient that his or her response is common, is not necessarily pathological, and that most people soon overcome their fear and return to a normal pre-trauma level of functioning. The physician’s goals should include reinforcing the patient’s strengths, encouraging use of existing support networks, offering referral for counseling if it is needed (eg, for more persistent and significant symptoms that impair function), offering a follow-up appointment within 2 to 4 weeks to monitor symptom progression and severity, and educating the patient to look for warning signs of a greater problem that will require a more immediate intervention (eg, suicidal ideation, significant impairment in functioning, or symptoms that do not improve or worsen over an additional 2 to 3 weeks). In general, the sooner the individual is able to return to his or her normal level of functioning and routine, the less likely it is that he or she will develop chronic, debilitating symptoms of PTSD.1,12,20,21
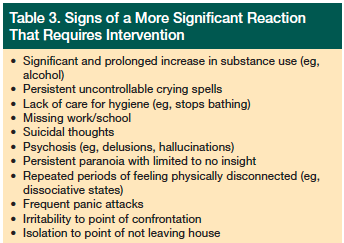 There is no clear data at this time to indicate that undergoing brief counseling immediately after a trauma will prevent the average or “normal” person (ie, non-pathological symptom-exposed person) from developing PTSD.13-15,23 Data indicate that providing counseling to “normal” individuals after a trauma actually leads to an increase in reported PTSD symptoms at the 3-month, 6-month, and 1-year marks, compared with normal individuals who did not undergo post-event counseling.13-17 Individuals who present with acute stress disorder, which is often a precursor to PTSD but does not always progress to PTSD, tend to benefit from psychotherapy (eg, cognitive behavioral treatment) in close proximity to the trauma, but additional studies are still needed to further define the subpopulations who will benefit the most.13,15,17 As with the use of medications, where perceived benefits outweigh risks, the same model holds true for engaging in psychotherapy. In the early stages, only individuals with clear symptoms who are having difficulty returning to their previous level of normal functioning should be referred for therapy (Table 3). The final article in this series, which will be published in the September issue of the journal, will delve into further detail about psychotherapeutic interventions for treating PTSD and how these techniques can be successfully combined with medication when needed.
There is no clear data at this time to indicate that undergoing brief counseling immediately after a trauma will prevent the average or “normal” person (ie, non-pathological symptom-exposed person) from developing PTSD.13-15,23 Data indicate that providing counseling to “normal” individuals after a trauma actually leads to an increase in reported PTSD symptoms at the 3-month, 6-month, and 1-year marks, compared with normal individuals who did not undergo post-event counseling.13-17 Individuals who present with acute stress disorder, which is often a precursor to PTSD but does not always progress to PTSD, tend to benefit from psychotherapy (eg, cognitive behavioral treatment) in close proximity to the trauma, but additional studies are still needed to further define the subpopulations who will benefit the most.13,15,17 As with the use of medications, where perceived benefits outweigh risks, the same model holds true for engaging in psychotherapy. In the early stages, only individuals with clear symptoms who are having difficulty returning to their previous level of normal functioning should be referred for therapy (Table 3). The final article in this series, which will be published in the September issue of the journal, will delve into further detail about psychotherapeutic interventions for treating PTSD and how these techniques can be successfully combined with medication when needed.
Pharmacological Management of PTSD
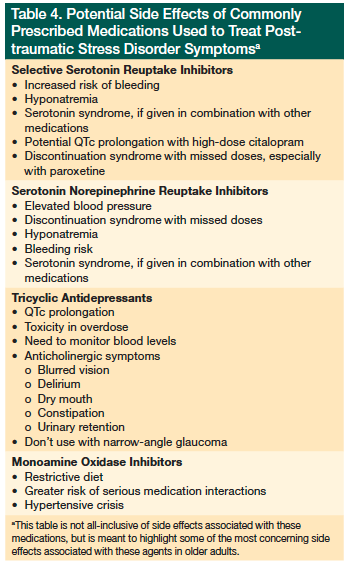 To date, no medications have been found to prevent the development of PTSD after exposure to a trauma.1 However, clinicians have several options in treating the symptoms of PTSD with medication once it occurs. The traditional first-line class of medications has been antidepressants. Use of other agents, such as antipsychotics, antiepileptics, and novel off-label uses of other nontraditional psychiatric classes of medication, such as blood pressure treatments, are being used as adjunctive therapy for PTSD symptoms. What follows is a brief overview of these agents and considerations before prescribing them to older adults (Table 4).
To date, no medications have been found to prevent the development of PTSD after exposure to a trauma.1 However, clinicians have several options in treating the symptoms of PTSD with medication once it occurs. The traditional first-line class of medications has been antidepressants. Use of other agents, such as antipsychotics, antiepileptics, and novel off-label uses of other nontraditional psychiatric classes of medication, such as blood pressure treatments, are being used as adjunctive therapy for PTSD symptoms. What follows is a brief overview of these agents and considerations before prescribing them to older adults (Table 4).
Antidepressants
Currently, the selective serotonin reuptake inhibitors (SSRIs) paroxetine and sertraline have been approved by the US Food and Drug Administration (FDA) for the treatment of PTSD once symptoms have developed.17 Although these are the only two medications to have FDA approval for the specific indication of PTSD, many other medications have demonstrated efficacy in the treatment of PTSD in research, including other SSRIs, tricyclic antidepressants, monoamine oxidase inhibitors, and serotonin-norepinephrine reuptake inhibitors (SNRIs).1,17,24-26 In general, SSRIs are considered the pharmacological first-line treatment for PTSD because they treat symptoms for all three PTSD symptom clusters (ie, reexperience, avoidance, increased arousal), they generally have the most benign side-effect profile of any group of antidepressants with equal efficacy, and they are effective in treating frequently occurring comorbid conditions, such as depression, general anxiety, and obsessive-compulsive disorder. 1,17,24-26 In addition, neuroimaging studies indicate that SSRIs, along with some other classes of antidepressant medications (eg, SNRIs), may treat PTSD by strengthening the cortical pathways, thereby helping to diminish fear responses.27
Benzodiazepines
Although traditionally benzodiazepines have been used for symptomatic relief of anxiety, their long-term use is not recommended for the treatment of PTSD due to their addictive nature, their potential to induce rebound anxiety when discontinued (eg, particularly short-acting agents such as alprazolam), and, to date, a lack evidence that they produce any positive neurocortical changes, such as those seen with the antidepressants.26 There are even studies suggesting that receiving benzodiazepines shortly after being exposed to a trauma may actually increase the risk of developing PTSD due to the benzodiazepine’s effects on normal stress hormone responses.28 In addition, the use of benzodiazepines in the elderly is associated with an increase in mortality due to falls and fractures and an increased risk for delirium and memory impairment. Their use in the elderly should be well conceived and judicious.29,30
Considerations Before Starting Pharmacological Treatment of PTSD in the Elderly
When trying to decide which treatment is best for an elderly individual with PTSD, several factors need to be taken into consideration. Clinicians need to remember that not every exposure to a trauma results in PTSD; 70% to 90% do not, and not every case of PTSD becomes chronic (50% resolve within 3 to 6 months, with only about 30% lasting longer than 1 year).1-3 In many cases, PTSD occurs in the context of other psychiatric conditions/symptoms, such as depression, anxiety, panic disorder, and/or substance abuse; thus, treatment of one symptom complex alone rarely results in substantial long-term improvement.
Some newer studies and metanalyses call into question the effectiveness of monotherapy with SSRIs or SNRIs for the treatment of PTSD and encourage polypharmacy for targeting general symptoms, as well as specific symptoms, such as sleep disturbance.31,32 Other psychiatric medications, such as mood stabilizers/antiepileptics (eg, lamotrigine, topiramate), atypical antidepressants (eg, trazodone), and atypical neuroleptic medications (eg quetiapine, risperidone), as well as some somatic medications, such as alpha blockers (eg, prazosin, clonidine) and beta blockers (eg, propranolol), are being used as adjunct or “novel” therapies.17,31,32 Although there may be a time and place for a polypharmaceutical approach to the treatment of PTSD, caution is advised, especially in a geriatric population, which is more susceptible to the side effects of these medications, as well as potential drug-drug interactions, such as increased risk of delirium and variances in metabolism.18,29,30
What is surprising is that even though medications effectively treat PTSD symptoms, they are underutilized in many treatment groups, especially the elderly. In a study by Mohamed and Rosenheck33 that involved older VA patients (eg, age >45 years) with PTSD, an inverse relationship between age and medication treatment was observed; for example, the older an individual was, the less likely he or she was to receive pharmacological treatment for PTSD. The authors concluded, “Older veterans diagnosed with PTSD appear to receive conservative, cautious treatment [which] may reflect some degree of undertreatment.”33
Conclusion
PTSD is a complex, multifactorial disorder, and one in which individual presentations vary greatly. In the absence of a cure for PTSD, treatment must be individualized and targeted to improve quality of life. As previously discussed, PTSD often occurs in the presence of physical and psychiatric comorbidities, so a single approach to treatment is rarely effective in the long-term. This article only discussed the considerations for managing PTSD and for deciding which, if any, medication to prescribe to help treat PTSD symptoms in older adults. Our subsequent article will discuss psychotherapeutic approaches as well as demonstrate that there is strong evidence that supports the combined use of psychopharmacology and psychotherapy in the treatment of refractory PTSD.
References
1. Ursano RJ, Bell C, Eth S, et al; Work Group on Acute Stress Disorder and Posttraumatic Stress Disorder. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1670530. Published November 2004. Accessed July 18, 2013.
2. Hall RC, Hall RC. Detection of malingered PTSD: an overview of clinical, psychometric, and physiological assessment: where do we stand? J Forensic Sci. 2007;52(3):717-725.
3. Hall RC, Hall RC. Malingering of PTSD: forensic and diagnostic considerations, characteristics of malingerers and clinical presentations. Gen Hosp Psychiatry. 2006;28(6):525-535.
4. Hall RC, Hall RC, Chapman MJ. Effects of terrorist attacks on the elderly - part I: medical and psychiatric complications of bombings and biological, chemical, and nuclear attacks. Clinical Geriatrics. 2006;14(8):26-35.
5. Hall RC, Hall RC, Chapman MJ. Effects of terrorist attacks on the elderly - part II: posttraumatic stress, acute stress, and affective disorders. Clinical Geriatrics. 2006;14(9):17-24.
6. Busuttil W. Presentations and management of Post Traumatic Stress Disorder and the elderly: a need for investigation. Int J Geriatr Psychiatry. 2004;19(5):429-439.
7. McHugh PR, Treisman G. PTSD: a problematic diagnostic category. J Anxiety Disord. 2007;21(2):211-222.
8. Osei-Boamah E, Pilkins BJ, Gambert SR. Post-traumatic stress disorder: a historical perspective of an evolving diagnosis. Clinical Geriatrics. 2013;21(6). Published online June 25, 2013.
9. Nucifora FC, Hall RC, Everly GS. Reexamining the role of the traumatic stressor and the trajectory of posttraumatic distress in the wake of disaster. Disaster Med Public Health Prep. 2011;suppl 2:S172-S175.
10. Hall RC, Hall RC. The 1995 Kikwit Ebola outbreak—model of virus properties on system capacity and function: a lesson for future viral epidemics. Am J Disaster Med. 2007;2(5):270-276.
11. Hall RC, Hall RC, Chapman MJ. The 1995 Kikwit Ebola outbreak: lessons hospitals and physicians can apply to future viral epidemics. Gen Hosp Psychiatry. 2008;30(5):446-452.
12. Tucker P, Ng A. Helping adults after disaster strikes. In: Hall RC, Ng A, Norwood AE, eds. Disaster Psychiatry Handbook. Arlington, VA: American Psychiatric Association Committee on Psychiatric Dimensions of Disaster, 2004:20-28.
13. Kornør H, Winje D, Ekeberg Ø, et al. Early trauma-focused cognitive-behavioural therapy to prevent chronic post-traumatic stress disorder and related symptoms: a systematic review and meta-analysis. BMC Psychiatry. 2008;19(8):81-99.
14. Roberts NP, Kitchiner NJ, Kenardy J, Bisson J. Multiple session early psychological interventions for the prevention of post-traumatic stress disorder. Cochrane Database Syst Rev. 2009;(3):CD006869.
15. Roberts NP, Kitchiner NJ, Kenardy J, Bisson JI. Early psychological interventions to treat acute traumatic stress symptoms. Cochrane Database Syst Rev. 2010;(3):CD007944.
16. Aulagnier M, Verger P, Rouillon F. Efficiency of psychological debriefing in preventing post-traumatic stress disorders. Rev Epidemiol Sante Publique. 2004;52(1):67-79.
17. Sharpless BA, Barber JP. A clinician’s guide to PTSD treatments for returning veterans. Prof Psychol Res Pr. 2011;42(1):8-15.
18. Hall RC, Hall RC, Chapman M. Identifying geriatric patients at risk for suicide and depression. Clinical Geriatrics. 2003;11(10):36-44.
19. Durai UN, Chopra MP, Coakley E, et al. Exposure to trauma and posttraumatic stress disorder symptoms in older veterans attending primary care: comorbid conditions and self-rated health status. J Am Geriatr Soc. 2011;59(6):1087-1092.
20. Hall RCW, Hall RCW, Chapman MJ. Emotional and psychiatric effects of weapons of mass destruction in first responders. In: Ursano RJ, Norwood AE, Fullerton CS, eds. Bioterrorism: Psychological and Public Health Interventions. Cambridge, UK: Cambridge University Press; 2004:250-273.
21. Hall RCW, Hall RCW, Chapman MJ. Psychiatric effects of terrorism: medical and societal implications of recent attacks. In: Linden EV, ed. Focus on Terrorism. Vol 9. New York, NY: Nova Science; 2007:237-255.
22. Effects of traumatic stress after mass violence, terror, or disaster: normal reactions to an abnormal situation. US Department of Veterans Affairs Website. http://www.ptsd.va.gov/professional/pages/stress-mv-t-dhtml.asp. Updated December 20, 2011. Accessed August 1, 2013.
23. Kar N. Cognitive behavioral therapy for the treatment of post-traumatic stress disorder: a review. Neuropsychiatr Dis Treat. 2011;7:167-181.
24. Stein DJ, Ipser JC, Seedat S. Pharmacotherapy for post traumatic stress disorder (PTSD). Cochrane Database Syst Rev. 2006;(1):CD002795.
25. Ipser JC, Stein DJ. Evidence-based pharmacotherapy of post-traumatic stress disorder (PTSD). Int J Neuropsychopharmacol. 2012;15(6):825-840.
26. Bisson JI. Post-traumatic stress disorder. Clin Evid (Online). 2010 Feb 3;2010. pii: 1005.
27. Fani N, Ashraf A, Afzal N, et al. Increased neural response to trauma scripts in posttraumatic stress disorder following paroxetine treatment: a pilot study. Neurosci Lett. 2011;491(3):196-201.
28. Matar MA, Zohar J, Kaplan Z, Cohen H. Alprazolam treatment immediately after stress exposure interferes with the normal HPA-stress response and increases vulnerability to subsequent stress in an animal model of PTSD. Eur Neuropsychopharmacol. 2009;19(4):283-295.
29. Hall RC, Hall RC, Chapman MJ. Central serotonin syndrome: part I - causative agents, presentation, and differential diagnosis. Clinical Geriatrics. 2007;15(12):18-25.
30. Hall RC, Hall RC, Chapman MJ. Anticholinergic syndrome: presentations, etiological agents, differential diagnosis, and treatment. Clinical Geriatrics. 2009;17(11):22-28.
31. Bajor LA, Ticlea AN, Osser DN. The Psychopharmacology Algorithm Project at the Harvard South Shore Program: an update on posttraumatic stress disorder. Harv Rev Psychiatry. 2011;19(5):240-258.
32. Shad MU, Suris AM, North CS. Novel combination strategy to optimize treatment for PTSD. Hum Psychopharmacol. 2011;26(1):4-11.
33. Mohamed S, Rosenheck R. Pharmacotherapy for older veterans diagnosed with posttraumatic stress disorder in Veterans Administration. Am J Geriatr Psychiatry. 2008;16(10):804-812.
Disclosures: The authors report no relevant financial relationships.
Address correspondence to: Ryan C. Hall, MD, 2500 West Lake Mary Blvd, Suite 219, Lake Mary, FL 32746; dr.rcwhall@live.com.