
Are You Equipped to Treat Tobacco Dependence?
ABSTRACT: Although tobacco use is the leading cause of preventable death in the United States, tobacco dependence remains an undertreated condition. Brief interactions with providers are both a cost-effective and clinically meaningful intervention, but low provider self-efficacy is a limiting factor in tobacco treatment. Tobacco dependence consultative services fit with the way other chronic conditions are managed, and may improve provider willingness to engage with this undertreated problem by improving self-efficacy. This article outlines effective tobacco treatment techniques, including motivational interviewing and pharmacotherapy.
Tobacco use is the leading cause of preventable death in the United States, claiming 480,000 lives per year.1 Educational public health campaigns and the emergence of effective treatments have decreased the prevalence of smoking over the last several decades, yet 18.1% of Americans still smoke.2 In clinical practice, this translates to almost 1 in 5 patients who are struggling with tobacco dependence and who may continue to smoke despite awareness of their health risks.
____________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
FDA Proposes to Expand Regulation of Tobacco
Quitting Smokeless Tobacco Extends Life Expectancy Post-Heart
____________________________________________________________________________________________________________________________________________________________________
Physicians identify tobacco use as a primary concern in their practice,3 and clear tobacco treatment guidelines exist to facilitate counseling and guide the prescription of medications.4 Even brief interventions by physicians have been shown to be both clinically meaningful and cost-effective in reducing the burden of tobacco.5-7
Yet, tobacco dependence remains an undertreated condition when compared with similarly prevalent, chronic conditions that are exacerbated by smoking—eg, hypertension, cardiovascular disease, and asthma.8 In a 2005-2007 survey, only 4.4% of primary care visits resulted in tobacco-specific medication prescriptions, while other chronic conditions were 16 to 29 times more likely to be treated with condition-specific medication.8
If clinicians identify tobacco dependence as a priority issue with effective treatments, why do they not intervene consistently?
Improving Tobacco Use Counseling
Studies suggest that tobacco use counseling is limited by the physicians’ sense of helplessness and their lack of faith in their own ability to reach abstinence goals with their patients—they expect negative results from their counseling efforts and experience low office support for tobacco treatment.6,9
Efforts to improve tobacco treatment in primary care settings should focus on increasing the clinicians’ self-efficacy. One effective approach may be to improve clinical support services within the systems that clinicians work. The management of any chronic illness may require consultative support to address the needs of patients with complex problems. While clinicians may be able to take advantage of community-based tobacco dependence resources, clinicians may perceive these resources as limited in their effectiveness, especially for patients with complex medical conditions.10
When deciding whether or not to refer, it is the quality of medical care the patient will receive that most influences provider referral decisions.11 Clinicians also cited personal knowledge of the specialist or service, perceived usefulness to the patient and beyond the scope of the clinician’s practice, and the likelihood of successful outcome and patient satisfaction.12
Clinicians are generally risk-aversive when making referral decisions and refer more frequently when they feel comfortable explaining the nature of the service.13 Expectations for shared care are common and have an important impact on the satisfaction with the referral outcome.14 Primary care practices that set up consultative services through dedicated tobacco-dependence appointments, in a manner similar to the provision of geriatric or sports medicine services, may help empower their whole system to address tobacco dependence during patient visits.
What is Tobacco Dependence?
A primary reason for the clinician’s low expectation is the paradox of the smoker who wants to quit, but who resists treatment. Unfortunately, this scenario is frequently encountered because tobacco dependence is a disorder of the motivation systems of the brain, manifesting as a poorly-controlled compulsion to continue smoking.
Ambivalence about quitting and compulsion to smoke are not reasons to avoid treatment. Instead they should be considered cardinal signs of underlying motivational disorders of dependence and are indications for the physician to initiate tobacco dependence treatment.15,16 Readiness to quit is not a prerequisite for providing tobacco treatment.
The compulsion to smoke can outweigh the immense societal pressures to quit. Nicotine binds to the cholinergic receptors on the ventral tegmental area (VTA) in the brain and functions as an imposter safety signal, hijacking the brain’s basic survival instincts.17 The VTA sends projections to the emotional centers of the brain to create a visceral sense of safety and correctness.
Over the long-term, this process can alter the brain’s function and structure such that the decision to forego smoking results in an amplified dysphoric emotional response, impulsive motivation to resume the behavior, and a progressively narrowed range of available coping mechanisms. As a result, the brain interprets the absence of nicotine akin to a threat to safety—creating visceral feelings of uneasiness and anxiety that are not quieted until the next puff of the cigarette.
As a device, the cigarette is the most efficient at delivering the free-base form of nicotine, a highly reactive and addictive form of the drug. The free-base nicotine inhaled through smoke can travel from the lungs to the brain in a matter of seconds, creating a large spike in tegmental nicotine concentration and high addictive potential.18,19 The effects of nicotine may not be apparent to people around the smoker because nicotine creates neither hedonic effects (eg, drunkenness or euphoria), nor does it produce a similarly dramatic and visible withdrawal. This may lead nonsmokers to assume that nicotine’s grip is weaker than other drugs of abuse.
Several animal studies since the 1980s have documented nicotine’s ability to induce powerful and persistent drug-seeking behavior.20-22 Researchers noted that the punishment of drug-seeking behavior or substitution of saline for cocaine, amphetamine, or morphine can reliably reduce self-administration behaviors,23,24 but the drug-seeking behavior produced by nicotine is much stronger and more persistent.25,26 Simply put, smokers experience a compulsion to use nicotine that is often impervious to punishment and more powerful than the compulsion produced by most other drugs.
As a result, the patient’s anticipation of withdrawal or even a discussion of abstinence can result in amplified emotional distress, which manifests as resistance to a clinician’s advice. This avoidance may be as subtle as a patient saying, “I’ll quit, but not today,” or as overt as “I don’t want to quit.” While the clinician may focus on discussing the reasons to quit, the smoker struggles to overcome the underlying motivation not to quit.
When clinicians are able to set aside the traditional method of increasing patient motivation to quit in favor of a strategy that focuses on easing distress and removing obstacles, they increase the likelihood of a successful interaction and a more productive therapeutic relationship. The keys to managing the patient’s anxiety and compulsion are motivational interviewing and effective pharmacotherapy.
(Understanding Tobacco Dependence Treatment and Pharmacotherapy on next page)
Understanding Tobacco Dependence Treatment
Taking a History
As with any patient interaction, a thorough history is the most important tool in the tobacco treatment consultant’s toolkit. At a minimum, the history for tobacco treatment should include the following:
• Duration of smoking in years
• Brief assessment of anxiety, depression, and stress
• Presence of a household smoker
• Other medical conditions, psychiatric conditions, or addictions
• Past attempts to quit—including when they occurred, the level of success, withdrawal symptoms, methods used, and triggers that led to relapse
• An assessment of the level of dependence
o Time to first cigarette (TTFC). This assessment gives the clinician an indication of the intensity of the patient’s need for nicotine upon awakening in a state of withdrawal.27,28 A TTFC of 30 minutes or less suggests moderate dependence, while a TTFC of 5 minutes or less qualifies as severe dependence.29
o Cigarettes per day (CPD). Though it is recommended that clinicians ask about the CPD, this gives only a very rough estimate of dependence and can provide an incomplete picture.30 Instead, qualitative descriptions of smoking intensity may be more useful.31 For example, a patient using 2 CPD may still be displaying signs of significant compulsion if their pattern is to take multiple aggressive puffs before extinguishing the cigarette in anticipation of reigniting and redosing later.
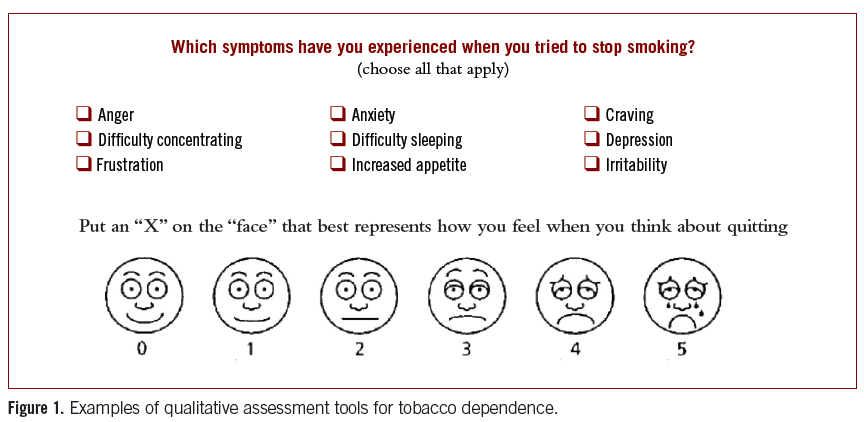
o Qualitative measures. Assessments of the patient’s dependence over time will necessarily include a number of qualitative measures, such as the patient’s description of the subjective distress resulting from compulsive behavior or the nature of any obsessive thoughts during periods of abstinence (Figure 1).
____________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Does Smoking Increase the Risk of Oral HPV?
CVS Pharmacy Will No Longer Sell Cigarettes
____________________________________________________________________________________________________________________________________________________________________
Motivational Interviewing
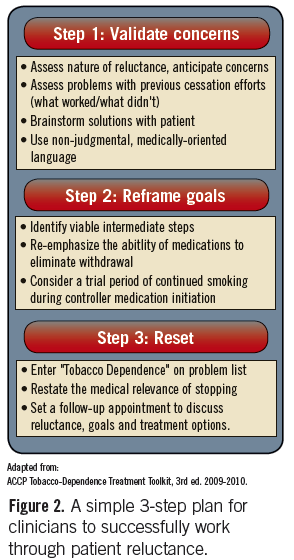
Motivational interviewing is a directed method of improving the impact of a patient’s own internal motivations to change by helping to resolve their ambivalence toward change (Figure 2). It is a critical tool for the tobacco treatment consultant, as it facilitates effective behavioral counseling and helps address the concerns that patients express about tobacco treatment medications.32
Motivational interviewing involves active listening to get to the patient’s “back story” in order to understand the underlying incentives and disincentives for tobacco treatment—ie, the motivations to quit and the motivations not to quit. This process requires the consultant to suspend moral judgment and avoid attempts to convince the patient to pursue a particular treatment. Drawing the patients’ rationalizations out and into words allows the patient to hear the inconsistencies in their own thinking, rather than the consultant pointing it out and risking shaming the patient.33
One of the biggest barriers in tobacco treatment is patients’ resistance to medication. This resistance is partly a manifestation of the addiction itself and partly due to common myths about the safety of these medications. Motivational interviewing allows the patient to feel comfortable bringing up their concerns about the medications. The consultant can then validate the patient’s position, while simultaneously undermining the source of patient concerns. This non-confrontationalapproach increases the likelihood that the patient will trust the consultant’s advice and try the medication.
Pharmacotherapy
After deciding to start the patient on medication, use these strategies to encourage adherence.
1. Start at a high dose. Tobacco treatment works best using an asthma control paradigm—start the patient on high doses and combinations of medication to allow the consultant to gain control of the underlying pathophysiology early, and then taper medication dosage over time.34,35 This is preferable to the blood pressure paradigm of titrating—ie, starting at a low dose of medication and increasing only as needed.
2. Avoid underdosing. Fear of overdose frequently limits patient willingness to use nicotine replacement therapy (NRT). However, keep in mind that nicotine delivery by NRT is much less efficient and more gradual than nicotine delivery from the cigarette, so it can be challenging to achieve a sufficient dose.36
For most patients, the 21 mg patch would be most suitable to start, but may still be inadequate for heavy smokers.36 Several studies have suggested safety and efficacy of using high-dose transdermal nicotine in 42 mg to 63 mg patches, though these studies failed to show statistical significance in long-term abstinence rates.37
3. Use combination medication. Another similarity between the treatment of asthma and tobacco is the use of a combination of controller and reliever medications. The patch delivers a steady, low dose of nicotine over a 24-hour period and can be used as a controller medication to help prevent cravings. The nicotine gum, lozenge, inhaler, or nasal spray can be used as a reliever medication to help manage breakthrough cravings.38
Many clinicians and patients fear the possibility of nicotine overdose with combination nicotine replacement, primarily because of concern over the impact of continued smoking. However, smokers unknowingly adjust their smoke intake downward to achieve baseline nicotine levels, and not more.39,40 At minimum, patients receiving nicotine replacement while continuing to smoke will reduce the amount of nicotine required from cigarettes, and consequently decrease their smoke-related health risk. Bupropion and varenicline may also be used in combination with reliever NRT for improved management of cravings.7,41-44
4. Embrace an extended pretreatment interval. The intense focus on cessation has resulted in treatment models where patients start treatment on the day of, or shortly before, abstinence begins. However, the tobacco dependence treatment requires a number of preparatory steps that might be taken in order to facilitate abstinence down the line.
One method of minimizing anxiety and improving the chances of medication adherence is to introduce the medication during the period prior to anticipated abstinence, also referred to as the pretreatment period. For example, a pretreatment plan to reduce patient anxiety may start with the recommendation to start taking the pill twice per day and keep smoking initially. Once the medication has a chance to work on the brain, a new strategy can be determined at the follow-up in 3 to 4 weeks.
This approach helps the patient feel more comfortable using the medication, while increasing the efficacy of treatment. Extended pretreatment periods of 3 to 4 weeks of varenicline have been associated with higher short-term abstinence rates than the recommended 1-week of pretreatment.45-47 Despite current recommendations to start nicotine on a quit date and the public’s general fear of smoking while on the patch, there is evidence to suggest that pretreatment with the patch is both safe and efficacious in promoting abstinence.48,49
5. Avoid deadlines. The primary goal should always be to manage the compulsion to smoke, rather than strictly to achieve abstinence. Many patients require more time than the traditional 8 to 10 weeks of NRT and there is no reason for artificial deadlines.7 In fact, longer patch usage has been associated with improved long-term abstinence outcomes and attenuation of weight gain.50 Smokers who use varenicline for 6 months instead of 3 months are more likely to achieve long-term abstinence51,52 and emerging evidence suggests that 1 year of treatment may be even more beneficial than 6 months of treatment.53
The best way to determine the duration of treatment is to assess the patient’s dependence, management of the compulsion, and level of struggle. For example, if a patient has been abstinent for weeks prior to a follow-up visit, but admits to dreaming about cigarettes or eating compulsively, continued treatment might be necessary in order to avoid relapse. In this case, ease the patient’s concerns and reassure the patient of the goals of treatment and the safety of continuing the medication.
Tobacco dependence should be treated as a chronic disease in which clinicians see patients regularly to manage ongoing issues. When tobacco treatment services are established within the chronic disease management model, systems improve both their efficiency and the effectiveness of their interventions. The availability of tobacco dependence consultative services fits with the way other chronic conditions are managed, and may improve provider willingness to engage with this undertreated problem by improving self-efficacy.
If there is no such service available to your practice, talk to the decision-maker in your practice about developing an in-house tobacco treatment clinic or identify a local tobacco specialist to consult. If you choose to develop a tobacco treatment consultative practice, consider a Tobacco Treatment Specialist training, which is specifically designed to help providers develop directorship-level skills in tobacco dependence treatment.
Danielle Peereboom, MPH, is a certified master tobacco treatment specialist at the University of Pennsylvania’s Comprehensive Smoking Treatment Program. She conducts visits to healthcare providers in Philadelphia to help improve tobacco treatment services at these practices.
Sarah Evers-Casey, MPH, is the associate director at the University of Pennsylvania’s Comprehensive Smoking Treatment Program. In addition to providing clinically-based tobacco treatment counseling, she coordinates all aspects of the program, including
community education and research.
Frank Leone, MD, MS, is a practicing pulmonologist and an associate professor of medicine at the University of Pennsylvania. He is the director of Penn’s Comprehensive Smoking Treatment Program and has been providing clinically-based tobacco treatment since 1993.
References:
1. National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention; 2014.
2. Agaku IT, King BA, Dube SR, Centers for Disease Control and Prevention (CDC). Current cigarette smoking among adults—United States, 2005-2012. MMWR Morb Mortal Wkly Rep. 2014;63(2):29-34.
3. McIlvain HE, Backer EL, Crabtree BF, Lacy N. Physician attitudes and the use of office-based activities for tobacco control. Fam Med. 2002;34(2):114-119.
4. Fiore M, Jaén C, Baker T, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: US Department of Health and Human Services. Public Health Service; 2008.
5. Maciosek MV, Coffield AB, Edwards NM, et al. Priorities among effective clinical preventive services: results of a systematic review and analysis. Am J Prev Med. 2006;31(1):52-61.
6. Solberg LI, Maciosek MV, Edwards NM, et al. Repeated tobacco-use screening and intervention in clinical practice: health impact and cost effectiveness. Am J Prev Med. 2006;31(1):62-71.
7. Cromwell J, Bartosch WJ, Fiore MC, et al. Cost-effectiveness of the clinical practice recommendations in the AHCPR guideline for smoking cessation. JAMA. 1997;278(21):1759-1766.
8. Bernstein SL, Yu S, Post LA, et al. Undertreatment of tobacco use relative to other chronic conditions. Am J Public Health. 2013;103(8):e59-65.
9. Garg A, Serwint JR, Higman S, et al. Self-efficacy for smoking cessation counseling parents in primary care: an office-based intervention for pediatricians and family physicians. Clin Pediatr (Phila). 2007;46(3):252-257.
10. Holtrop JS, Malouin R, Weismantel D, Wadland WC. Clinician perceptions of factors influencing referrals to a smoking cessation program. BMC Fam Pract. 2008;9:18.
11. Ludke RL. An examination of the factors that influence patient referral decisions. Med Care. 1982;
20(8):782-796.
12. Forrest CB, Nutting PA, Starfield B, von Schrader S. Family physicians’ referral decisions: results from the ASPN referral study. J Fam Pract. 2002;51(3):
215-222.
13. Holtgrave DR, Lawler F, Spann SJ. Physicians’ risk attitudes, laboratory usage, and referral decisions: the case of an academic family practice center. Med Decis Making. 1991;11(2):125-130.
14. Starfield B, Forrest CB, Nutting PA, von Schrader S. Variability in physician referral decisions. J Am Board Fam Pract. 2002;15(6):473-480.
15. Leone FT, Evers-Casey S. Behavioral interventions in tobacco dependence. Prim Care. 2009;36(3):
489-507.
16. Hyman SE. Addiction: a disease of learning and memory. Am J Psychiatry. 2005;162(8):1414-1422.
17. Leone FT, Evers-Casey S. Developing a rational approach to tobacco use treatment in pulmonary practice. Clin Pulm Med. 2012;19(2):53-61.
18. Henningfield JE, Stapleton JM, Benowitz NL, et al. Higher levels of nicotine in arterial than in venous blood after cigarette smoking. Drug Alcohol Depend. 1993;33(1):23-29.
19. Isaac PF, Rand MJ. Blood levels of nicotine and physiological effects after inhalation of tobacco smoke. Eur J Pharmacol. 1969;8(3):269-283.
20. Goldberg SR, Spealman RD, Risner ME, Henningfield JE. Control of behavior by intravenous nicotine injections in laboratory animals. Pharmacol Biochem Behav. 1983;19(6):1011-1020.
21. Goldberg SR, Henningfield JE. Reinforcing effects of nicotine in humans and experimental animals responding under intermittent schedules of IV drug injection. Pharmacol Biochem Behav. 1988;30(1):
227-234.
22. Henningfield JE, Goldberg SR. Nicotine as a reinforcer in human subjects and laboratory animals. Pharmacol Biochem Behav. 1983;19(6):989-992.
23. Grove RN, Schuster CR. Suppression of cocaine self-administration by extinction and punishment. Pharmacol Biochem Behav. 1974;2(2):199-208.
24. Smith S, Davis W. Punishment of amphetamine and morphine self-administration behavior. Psychol Rec. 1974;24:477-480.
25. Stolerman I. Animal models for nicotine dependence. In: Bock G, Goode J (eds). Understanding Nicotine and Tobacco Addiction: Novartis Foundation Symposium 275. Chichester, UK: John Wiley and Sons; 2006:17-35.
26. Le Foll B, Wertheim C, Goldberg SR. High reinforcing efficacy of nicotine in non-human primates. PloS One. 2007;2(2):e230.
27. Fagerström K. Time to first cigarette; the best single indicator of tobacco dependence? Monaldi Arch Chest Dis. 2003;59(1):91-94.
28. Baker TB, Piper ME, McCarthy D, et al. Time to first cigarette in the morning as an index of ability to quit smoking: implications for nicotine dependence. Nicotine Tob Res. 2007;9 Suppl 4:S555-S570.
29. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict. 1991;86(9):1119-1127.
30. McClure EA, Saladin ME, Baker NL, et al. Smoking topography and abstinence in adult female smokers. Addict Behav. 2013;38(12):2833-2836.
31. Brauer LH, Hatsukami D, Hanson K, Shiffman S. Smoking topography in tobacco chippers and dependent smokers. Addict Behav. 1996;21(2):233-238.
32. Britt E, Hudson SM, Blampied NM. Motivational interviewing in health settings: a review. Patient Educ Couns. 2004;53(2):147-155.
33. Amrhein PC, Miller WR, Yahne CE, et al. Client commitment language during motivational interviewing predicts drug use outcomes. J Consult Clin Psychol. 2003;71(5):862-878.
34. Sachs D, Leone F, Farber H, et al. American College of Chest Physicians Tobacco-Dependence Treatment Toolkit. 3rd ed. http://tobaccodependence.chestnet.org. Accessed November 8, 2014.
35. Henningfield JE, Fant RV, Buchhalter AR, Stitzer ML. Pharmacotherapy for nicotine dependence. CA Cancer J Clin. 2005;55(5):281-299.
36. Hurt RD, Dale LC, Offord KP, et al. Serum nicotine and cotinine levels during nicotine-patch therapy. Clin Pharmacol Ther. 1993;54(1):98-106.
37. Brokowski L, Chen J, Tanner S. High-dose transdermal nicotine replacement for tobacco cessation. Am J Health-Syst Pharm. 2014;71(8):634-638.
38. Rigotti NA. Treatment of tobacco use and dependence. N Engl J Med. 2002;346(7):506-512.
39. Benowitz NL, Zevin S, Jacob P. Suppression of nicotine intake during ad libitum cigarette smoking by high-dose transdermal nicotine. J Pharmacol Exp Ther. 1998;287(3):958-962.
40. Foulds J, Stapleton J, Feyerabend C, et al. Effect of transdermal nicotine patches on cigarette smoking: a double blind crossover study. Psychopharmacology (Berl). 1992;106(3):421-427.
41. Ebbert JO, Burke MV, Hays JT, Hurt RD. Combination treatment with varenicline and nicotine replacement therapy. Nicotine Tob Res. 2009;11(5):572-576.
42. Ebbert JO, Croghan IT, Sood A, et al. Varenicline and bupropion sustained-release combination therapy for smoking cessation. Nicotine Tob Res. 2009;11(3):234-239.
43. Stead LF, Lancaster T. Combined pharmacotherapy and behavioural interventions for smoking cessation. Cochrane Database Syst Rev. 2012;10:CD008286.
44. Koegelenberg CFN, Noor F, Bateman ED, et al. Efficacy of varenicline combined with nicotine replacement therapy vs varenicline alone for smoking cessation: a randomized clinical trial. JAMA. 2014;312(2):155-161.
45. Hajek P, McRobbie HJ, Myers KE, et al. Use of varenicline for 4 weeks before quitting smoking: decrease in ad lib smoking and increase in smoking cessation rates. Arch Intern Med. 2011;171(8):770-777.
46. Ashare RL, Tang KZ, Mesaros AC, et al. Effects of 21 days of varenicline versus placebo on smoking behaviors and urges among non-treatment seeking smokers. J Psychopharmacol. 2012;26(10):1383-1390.
47. Hawk LW, Ashare RL, Lohnes SF, et al. The effects of extended pre-quit varenicline treatment on smoking behavior and short-term abstinence: a randomized clinical trial. Clin Pharmacol Ther. 2012;91(2):172-180.
48. Rose JE, Herskovic JE, Behm FM, Westman EC. Precessation treatment with nicotine patch significantly increases abstinence rates relative to conventional treatment. Nicotine Tob Res Off J Soc Res Nicotine Tob. 2009;11(9):1067-1075.
49. Rose JE, Behm FM, Westman EC, Kukovich P. Precessation treatment with nicotine skin patch facilitates smoking cessation. Nicotine Tob Res. 2006;8(1):89-101.
50. Schnoll RA, Patterson F, Wileyto EP, et al. Effectiveness of extended-duration transdermal nicotine therapy: a randomized trial. Ann Intern Med. 2010;152(3):144-151.
51. Lee JH, Jones PG, Bybee K, O’Keefe JH. A longer course of varenicline therapy improves smoking cessation rates. Prev Cardiol. 2008;11(4):210-214.
52. Tonstad S, Tønnesen P, Hajek P, et al. Effect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trial. JAMA. 2006;296(1):64-71.
53. Evins AE, Cather C, Pratt SA, et al. Maintenance treatment with varenicline for smoking cessation in patients with schizophrenia and bipolar disorder: a randomized clinical trial. JAMA. 2014;311(2):145-154.
54. Prokhorov AV, Hudmon K, Marani S, et al. Engaging physicians and pharmacists in providing smoking cessation counseling. Arch Intern Med. 2010;170(18):1640-1646.
55. Association for the Treatment of Tobacco Use and Dependence (ATTUD) website. http://attudaccred.org/programs. Accessed October 27, 2014.
56. Manaker S, Krier-Morrow D, Pohlig C. Coding for Chest Medicine 2008: Pulmonary, Critical Care, Sleep. 12th ed. Northbrook, IL: American College of Chest Physicians; 2008.