
Adrenal Insufficiency
Christine Ellis, MD; Min Lee, MD; Emily Borne, MD; Michael Yafi, MD; and Julia Shelburne, MD, FAAP
A 14-year-old boy presented with a history of 3 days of nausea, vomiting, and abdominal pain. A review of systems was significant for chronic fatigue, weight loss, and increased skin pigmentation over the past 2 years, but the boy denied any known exposures to tuberculosis or HIV. Laboratory test results from the day of presentation revealed that he had a sodium level of 107 mEq/L, potassium level of 4.6 mEq/L, chloride level of 75 mEq/L, and carbon dioxide level of 17 mEq/L.
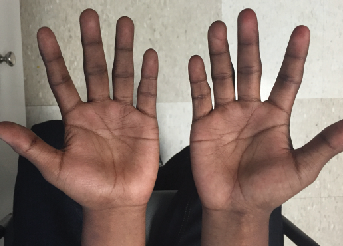
The boy’s initial heart rate was 87 beats/min, his respiratory rate was 16 breaths/min, and his blood pressure was 97/57 mm Hg. On physical examination, he had dry mucous membranes and generalized hyperpigmentation, including his gums, tongue, and creases on his palms and soles. In addition, he had diffuse mild-moderate tenderness on palpation of his abdomen without rebound or guarding. He was Tanner stage 4.



The patient was given a normal saline bolus, started on D5 1/2 Normal Saline at maintenance rate, and was given intravenous (IV) hydrocortisone 65 mg/m2. He was admitted to the hospital.
After the IV corticosteroid dose, laboratory test results showed adrenocorticotropic hormone (ACTH) of 1250 pg/mL and cortisol of 8.9 µg/mL. Test results for HIV, tuberculosis via purified protein derivative, anti-islet antibodies, anti-glutamic acid decarboxylase antibodies, anti-thyroid peroxidase antibodies, thyroglobulin, and adrenal antibodies were all negative. The results of the boy’s thyroid, lipid, and very long chain fatty acid panels were unremarkable.
Hydrocortisone was continued orally at 50 mg/m2/day, and fludrocortisone was added and titrated to 1.5 mg/day. To correct periodic hyponatremia, a sodium tablet of 1 g/day was added.
Over the next 5 days, the boy’s sodium levels slowly normalized, and his potassium level peaked at 5.9 mEq/L on his second day in the hospital. Once his sodium reached 137 mEq/L, his hydrocortisone was weaned to 20 mg/m2/day. He was diagnosed with primary adrenal insufficiency, confirmed by his very high ACTH level, and was discharged with close outpatient follow-up.
DISCUSSION
Adrenal insufficiency is a clinical condition of deficiency of adrenal glucocorticoids and possibly mineralocorticoids. This insufficiency can be primary (at the level of adrenal gland), secondary (ACTH deficiency from the pituitary gland), or tertiary (corticotropin-releasing hormone deficiency at the level of the hypothalamus).1,2 Primary adrenal insufficiency is also known as Addison disease, and it is most commonly caused by autoimmune destruction of the gland.3 Other causes include trauma, hemorrhage, infections such as tuberculosis and cytomegalovirus,3 and adrenoleukodystrophy.2,4 Adrenal unresponsiveness to ACTH causes adrenal insufficiency as a part of Allgrove syndrome, also known as Achalasia-Addisonianism-Alacrima syndrome (Triple A syndrome).5
Clinical presentation of patients with adrenal insufficiency is related to the deficiency of cortisol and aldosterone secretion and its metabolic effects of hypoglycemia, hyponatremia, and hyperkalemia,3 though hyperkalemia is not a universal feature.6 Symptoms of adrenal insufficiency include chronic fatigue, muscle weakness, nausea, abdominal pain, vomiting, weight loss, and headache.3
Adrenal crisis is the sudden worsening of adrenal insufficiency symptoms, including severe hypotension and dehydration, and it can be life-threatening.3 In primary adrenal insufficiency, chronic elevation of ACTH may be associated with elevation of melanocyte-stimulating hormones.7 This condition may cause hyperpigmentation of skin and of
mucosal membranes.
The diagnosis of adrenal insufficiency is suspected as a result of clinical and laboratory findings (ie, hyponatremia, hyperkalemia, hypoglycemia, low baseline cortisol level, and high ACTH levels).1,3,6 An ACTH stimulation test may be needed to confirm suboptimal cortisol reserve.3,6 Once the diagnosis of adrenal insufficiency is confirmed, the etiology should be sought.
Treatment for adrenal insufficiency depends on replacement of adrenal hormones (cortisol, aldosterone), use of medications (hydrocortisone or prednisone/prednisolone as well as fludrocortisone),3 and possible oral supplementation of salt. Education of patients and families to recognize and treat adrenal crisis with injectable stress doses of hydrocortisone is a critical part of the management plan.
Christine Ellis, MD, is a pediatrics resident at the University of Texas Health Science Center at Houston.
Min Lee, MD, is an internal medicine and pediatrics resident at the University of Texas Health Science Center at Houston.
Emily Borne, MD, is a pediatrics resident at the University of Texas Health Science Center at Houston.
Michael Yafi, MD, is an Associate Professor and Director of the Division of Pediatric Endocrinology at the University of Texas Health Science Center at Houston.
Julia Shelburne, MD, FAAP, is an Associate Professor of Pediatrics in the Division of Community and General Pediatrics at the University of Texas Health Science Center at Houston.
REFERENCES
1. Charmandari E, Nicolaides NC, Chrousos GP, et al. Adrenal insufficiency. Lancet. 2014;383(9935):2152-2167.
2. Auron M, Raissouni N. Adrenal insufficiency. Pediatric Rev. 2015;36(3):92-102.
3. National Institute of Diabetes and Digestive and Kidney Diseases. Adrenal insufficiency and Addison’s disease. http://www.nidk.nih.gov/health-infromation/health-topics/endocrine/adrenal-insufficiency-addisons-disease/pages/fact-sheet.aspx. Accessed May 31, 2016.
4. Nascimento M, Rodrigues N, Espada F, Fonseca M. Adrenoleukodystrophy: a forgotten diagnosis in children with primary Addison’s disease. BMJ Case Rep. 2012;pii: bcr2012006308.
5. Dumic M, Barišic N, Kusec V, et al. Long-term clinical follow-up and molecular genetic findings in eight patients with triple A syndrome. Eur J Pediatr. 2012;171(10):1453-1459.
6. Hsieh S, White PC. Presentation of primary adrenal insufficiency in childhood. J Clin Endocrinol Metab. 2011;96(6):E925-E928.
7. Coates PJ, McNicol AM, Doniach I, Rees LH. Increased production of α-melanocyte-stimulating hormone in the pituitary gland of patients with untreated Addison’s disease. Clin Endocrinol (Oxf). 1988;29(4):421-426.