
Peer Reviewed
An Unusual Presentation of Human Metapneumovirus Infection
Authors:
Tess Chamakkala, DO
Internal Medicine Resident, St. Luke’s University Hospital, Bethlehem, Pennsylvania
Manish Kumar, MD
Pediatrics Resident, Maimonides Children’s Hospital, Brooklyn, New York
Kamal Singh, MD
Chief of Pediatrics, Peconic Bay Medical Center, Riverhead, New York, and Assistant Professor of Pediatrics, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, New York
Sandeep A. Gandhi, MD
Infectious Diseases Consultant at Peconic Bay Medical Center, Riverhead, New York, and Associate Professor of Clinical Medicine, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, New York
Citation:
Chamakkala T, Kumar M, Singh K, Gandhi SA. An unusual presentation of human metapneumovirus infection. Consultant. 2020;60(1):29-30. doi:10.25270/con.2020.01.00008
A 15-month-old boy presented to the emergency department with multiple episodes of vomiting and a subjective fever for 2 days. His mother denied rhinorrhea or a cough in the child. The patient had no medical history. At presentation, his rectal temperature was 38°C, and his pulse was 145 beats/min. He was found to be mildly dehydrated and was admitted to the hospital.
Hospital course. On the day of admission, his temperature rose to 39.8°C, and he developed wheezing and coughing. An albuterol nebulizer provided some relief. On the second day of admission, his temperature rose to 40.3°C, and yellow diarrhea and intractable vomiting developed. He received a diagnosis of dehydration and viral gastroenteritis and was treated supportively with 5% dextrose in 0.33% normal saline and acetaminophen. On the third day, he was afebrile and began to tolerate breast milk and a regular diet. After a 4-day stay, the patient’s condition improved, and he was discharged home.
Laboratory tests. Results of a complete blood cell count showed a white blood cell count of 11,900/µL and a hemoglobin level of 11.0 g/dL. The lymphocyte count was elevated at 4300/µL, and the monocyte count was elevated at 1100/µL. Results of a rapid influenza antigen nasal swab test were negative. Chest radiography showed hyperinflated lungs and peribronchial cuffing (Figure). Blood culture results and urine culture results were normal. Urinalysis results were within normal limits, except for a ketone level of 40 mg/dL. Results of a rapid respiratory pathogen panel using polymerase chain reaction were positive for human metapneumovirus (HMPV) but negative for adenovirus, coronavirus, human enterovirus/rhinovirus, influenza, parainfluenza, and respiratory syncytial virus (RSV).
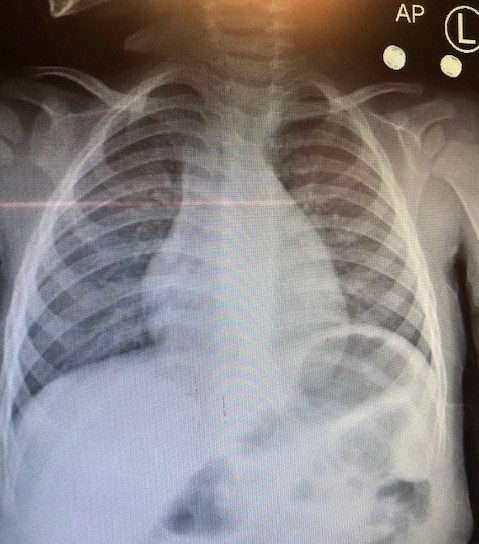
Figure. Chest radiograph showing hyperinflated lungs and peribronchial cuffing.
Discussion. HMPV is a respiratory pathogen that was first described in 2001 by researchers in the Netherlands.1 HMPV is in the Pneumoviridae family, which also includes RSV.2 HMPV infection presents clinically with many of the same signs and symptoms as RSV infection, and the diseases caused by either virus cannot be differentiated without laboratory testing.
Common clinical manifestations of HMPV infection are fever greater than 38°C, cough, rhinitis, wheezing, tachypnea, retractions, hypoxia (oxygen saturation <94%), and findings of infiltrates or hyperinflation on chest radiographs. HMPV can also manifest less commonly with otitis media or pharyngitis and rarely with encephalitis or conjunctivitis.3 Gastrointestinal tract symptoms such as the intractable vomiting in our 15-month-old patient are not a known manifestation of HMPV infection.
HMPV infections occur worldwide but are more common during winter in areas of temperate climate.4 The infections occur early in life; by age 5, almost all children have serum antibodies to HMPV.4 In addition, an estimated 1% to 5% of all childhood upper respiratory tract infections are caused by HMPV.4 Reinfection with HMPV after childhood can manifest ranging from a subclinical infection to pneumonia.4 More serious infections occur in immunocompromised patients.4
HMPV is most likely spread through secretions from coughing and sneezing, from close personal contact such as shaking hands, and from touching surfaces that have the virus on them and then touching the mouth, nose, or eyes.5 Treatment is currently supportive. However, ribavirin has been shown to be active against HMPV in vitro.6
- van den Hoogen BG, de Jong JC, Groen J, et al. A newly discovered human pneumovirus isolated from young children with respiratory tract disease. Nat Med. 2001;7(6):719-724.
- Amarasinghe GK, Bào Y, Basler CF, et al. Taxonomy of the order Mononegavirales: update 2017. Arch Virol. 2017:162(8):2493-2504.
- Crowe JE Jr. Human metapneumovirus. In: Kliegman RM, Stanton BF, St Geme JW III, Schor NF, eds. Nelson Textbook of Pediatrics. Vol 1. 20th ed. Philadelphia, PA: Elsevier; 2016:chap 261.
- Dolin R. Common viral respiratory infections. In: Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine. Vol 2. 19th ed. New York, NY: McGraw-Hill; 2014:chap 223.
- Human metapneumovirus (HMPV) clinical features. Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases, Division of Viral Diseases. https://www.cdc.gov/surveillance/nrevss/hmpv/clinical.html. Reviewed March 13, 2019. Accessed March 25, 2019.
- Wyde PR, Chetty SN, Jewell AM, Boivin G, Piedra PA. Comparison of the inhibition of human metapneumovirus and respiratory syncytial virus by ribavirin and immune serum globulin in vitro. Antiviral Res. 2003;60(1):51-59.