
Peer Reviewed
White Tongue
Authors:
Chantel T. Jacobs, MD
Recent Graduate, Bayfront Health St. Petersburg Family Medicine Residency Program, St. Petersburg, Florida
W. Michael Brown, MD
Associate Director, Bayfront Health St. Petersburg Family Medicine Residency Program, St. Petersburg, Florida
Citation:
Jacobs CT, Brown WM. White tongue. Consultant. 2019;59(10):319-320.
A 3-week-old boy presented with a white coating on his tongue for 1 week. He had been born to a healthy 34-year-old, gravida 1, para 1 mother whose prenatal course had been uncomplicated. The patient’s mother had tested positive for group B streptococcus (GBS) and received vancomycin, 1 g, 8 hours prior to spontaneous vaginal delivery.
At 2 weeks of age, the patient’s mother noticed a white coating on the neonate’s entire tongue (Figure 1) but was able to remove it easily. The following week, the coating became thicker and was not removable.

Figure 1. At 2 weeks of age, the patient’s tongue had a thick white coating.
The patient continued to drink without difficulty. Nystatin oral suspension, 100,000 U/mL, was prescribed and used for 14 days with no improvement of the white coating. Fluconazole oral suspension, 10 mg/mL, was then prescribed and used for 7 days with mild improvement (Figure 2). During this time, the patient remained free of diaper rash.
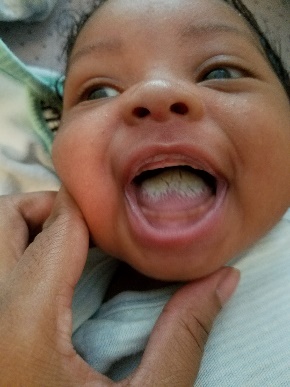
Figure 2. Mild improvement of the white tongue with the use of fluconazole.
Gentian violet was applied to the tongue soon after; the following day, the purple discoloration had disappeared (Figures 3-5).

Figure 3. Gentian violet, day 1.

Figure 4. Gentian violet, day 2.

Figure 5. Gentian violet, day 3.
Gentian violet was then applied a second time to the 6-week-old boy, and fluconazole was restarted the day after. Five days later, the white coating had lifted from the tongue and was removed (Figures 6-8). The patient completed 14 days of fluconazole.
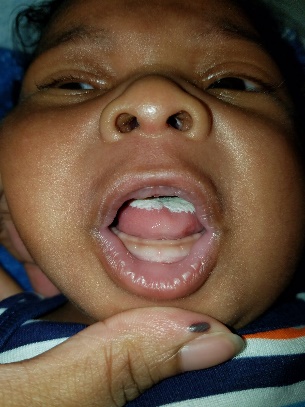
Figure 6. Slight edema of tongue and lifting of the white coating.
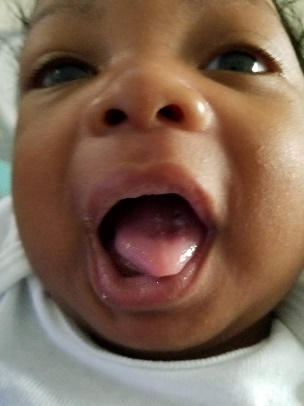
Figure 7. Significant improvement of the white tongue.
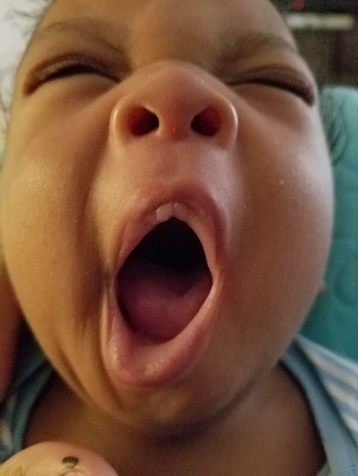
Figure 8. Complete resolution of the white tongue.
One week later, however, the white coating returned (Figure 9).
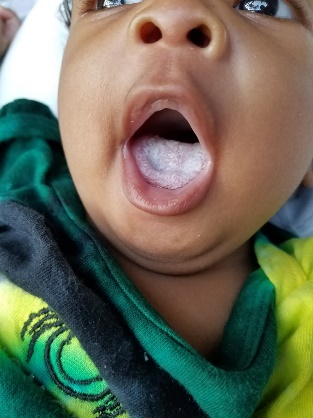
Figure 9. Moderate white coating of the tongue returned.
During the entire period, there had been no sign of diaper rash before or after antifungal treatment.
Diagnosis. Initially, it had been assumed that the patient had oral thrush given his symptoms. However, the presumed thrush had not improved with nystatin or fluconazole treatment. After applying gentian violet twice and restarting fluconazole a second time, the white coating resolved.
While being treated, the patient’s tongue was cultured for Candida albicans, and results were negative. His tongue was then cultured for bacteria, given that the patient’s mother had been GBS-positive and that the patient had been in the birth canal for 3 hours before delivery. Bacteria culture grew Escherichia coli. This positive culture was concerning; however, no other signs of infection were present. The patient’s mother also tested her breastmilk for yeast, since the patient was being strictly breastfed; the culture results was negative.
The patient continued to be free of diaper rash, which made oral thrush less likely because the 2 conditions usually present together. The patient remained afebrile and continued to drink breastmilk without difficulty. After many treatment courses and then the return of the white coating, the patient received a clinical diagnosis of white tongue.
Discussion. White tongue is a diagnosis of exclusion. This benign, painless condition may mimic many conditions such as oral thrush and results from hypertrophy of the filiform papillae on the surface of the tongue. The papillary structure provides a large surface area that allows the accumulation of oral debris and microorganisms.1 The tongue coating comprises bacteria, desquamated epithelial cells from the oral mucosa, leukocytes from periodontal pockets, blood metabolites, and nutrients.1
The normal oral flora consists of Actinomyces, Bacteroides, Fusobacterium, Peptostreptococcus, and Prevotella species, to name a few.2-4 E coli is not a normal part of the oral flora, and E coli infections of the tongue are rare.5 One study has identified psoriasin as an E coli-killing protein that is the main antimicrobial component of the healthy human tongue.5 The presence of psoriasin has been identified in the vernix caseosa, suggesting its possible role in protecting a child from E coli infection during birth.5 Therefore, the positive E coli culture from this patient’s tongue likely was a false-positive result.
White tongue is painless and self-limiting, and treatment is not necessary; however, gentle brushing of the tongue maybe helpful.
White tongue should be considered in the evaluation of an infant with a recurring white-coating of tongue that is resistant to treatment, especially in the absence of diaper rash, difficulty feeding, fever, or other signs of infection. As the infant gets older and produces more saliva, the white coating on the tongue will become less pronounced.
- Danser MM, Gómez SM, Van der Weijden GA. Tongue coating and tongue brushing: a literature review. Int J Dent Hyg. 2015;1(3):151-158.
- Dewhirst FE, Chen T, Izard J, et al. The human oral microbiome. J Bacteriol. 2010;192(19):5002-5017.
- Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;43(11):5721-5732.
- Wade WG. The oral microbiome in health and disease. Pharmacol Res. 2013;69(1):137-143.
- Meyer JE, Harder J, Sipos B, et al. Psoriasin (S100A7) is a principal antimicrobial peptide of the human tongue. Mucosal Immunol. 2008;1(3):239-243.