
Peer Reviewed
Erythema Multiforme Minor Secondary to Pesticide Exposure: A Case Series
AUTHORS:
Haowei Han, DO
Transitional Year Resident, Peconic Bay Medical Center–Northwell Health, Riverhead, New York
Sandeep A. Gandhi, MD
Infectious Diseases Consultant at Peconic Bay Medical Center–Northwell Health, Riverhead, New York, and Associate Professor of Clinical Medicine, New York Institute of Technology College of Osteopathic Medicine, Old Westbury, New York
Kaushik Manthani, DO
Program Director, Transitional Year Residency Program, Peconic Bay Medical Center–Northwell Health, Riverhead, New York
Jean Cacciabaudo, MD
Medical Director, Peconic Bay Medical Center–Northwell Health, Riverhead, New York
CITATION:
Han H, Gandhi SA, Manthani K, Cacciabaudo J. Erythema multiforme minor secondary to pesticide exposure: a case series [published online December 9, 2019]. Consultant360.
We report 3 cases of erythema multiforme (EM) minor in patients who presented to our facility within a single week. All of the patients denied having started new medications and denied having a history of sexually transmitted infections. However, all 3 did report recent exposure to a pesticide. Thus, we suspect that a pesticide was the culprit in these EM eruptions.
CASE 1
A 44-year-old man with a medical history of multiple sclerosis presented with a 4-day history of an extremely painful rash all over his body accompanied by subjective fever. The rash had started on his right thumb and had spread over his elbow, chest, face, feet, knees, ears, and the tip of his nose. He denied having mucosal lesions and urinary tract symptoms. He recalled that he had been walking barefoot outdoors after pesticides had been sprayed around his house.
Skin examination revealed well-demarcated, round, erythematous patches with plaques on his feet, knees, elbows, chest, face, and the tip of his nose. No mucosal lesions were noted. His temperature at admission was 38.9°C. His other vital signs were stable. Results of a metabolic panel and a complete blood cell count (CBC) were unremarkable, except for an elevated erythrocyte sedimentation rate (ESR). Results of syphilis tests were negative. The patient’s symptoms eventually resolved in the next 2 days without intervention.
CASE 2
A 55-year-old man with a medical history of metabolic syndrome presented with a 4-day history of an excruciatingly painful maculopapular rash that had started on his right hand and had progressed to his extremities, trunk, and face. He recalled that his county health department’s vector control unit had sprayed pesticides around his house before the flare. He had been prescribed doxycycline and fluocinolone ointment, 0.01%, by an outside dermatologist, and a biopsy had been done at that time. Nevertheless, his condition had progressively worsened.
His vitals were stable at presentation. Physical examination revealed numerous well-rounded, targetoid patches and slightly raised papules and plaques on his palms, soles, hands, feet, face, trunk, and extremities (Figure 1). No mucosal involvement was present, and no bullae or vesicles were noted. Results of a CBC revealed an elevated white blood cell count and an elevated ESR.

Figure 1. Well-defined, erythematous patches and slightly raised papules and plaques on the patient’s hands.
A punch biopsy of a lesion on his right forearm displayed superficial acute inflammation and separation of the keratinized epithelium. The basal cell layer showed focal edema and reactive epithelial changes. He was given topical triamcinolone cream, 0.1%, and oral prednisone, 20 mg. His condition resolved in the next 3 days.
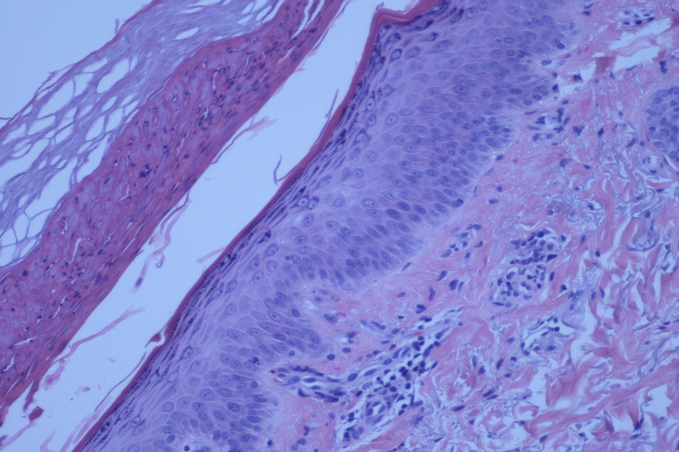
Figure 2. A deep biopsy revealed separation of the keratinized epithelium. The basal cell layer showed focal edematous changes.
CASE 3
A 26-year-old otherwise healthy man presented with 3-day history of a rash associated with intermittent fevers, vomiting, and a sore throat. The had rash started on his ankle and had spread to his feet, knees, hands, elbow, trunk, and face. He recalled that his county vector control unit had been spraying pesticides around his workplace. He reported that his relative who lives 5 blocks away from him also had developed a similar rash.
His temperature was 37.3°C. Other vital signs were within normal limits. Skin examination showed numerous, pink, round macules, vesicles, papules, and plaques on his hands, feet, palms, soles, back, neck, face, arms, and legs. There were a few lesions in his mouth and nose.



Figures 3-5. Pink, round macules, vesicles, papules, and plaques on the patient’s hands, feet, palms and soles.
Laboratory test results were unremarkable except for an elevated ESR. He was treated with oral prednisone, 60 mg, and topical triamcinolone ointment, 0.05%. The patient’s condition significantly improved after 24 hours of treatment. He was discharged with oral prednisone, 10 mg, and topical triamcinolone cream, 0.3%.
DISCUSSION
EM is a hypersensitivity reaction to infections or drugs. Infectious etiologies account for 90% of cases, with the other 10% caused by drugs.1 The most common trigger is herpes simplex virus. Other commonly reported triggers include Mycoplasma pneumoniae, sulfonamides, barbiturates, penicillin, and nonsteroidal anti-inflammatory drugs.2 M pneumoniae is a typical precipitator in the pediatric population. Rare cases of EM have been reported secondary to contact with laurel oil,3 or in association with other medical conditions such as autoimmune hepatitis and, possibly, systemic lupus erythematosus.4
EM most frequently affects people in their second or third decade. It is characterized by target lesions of usually less than 3 cm with a central, dusky area with a dark red inflammatory zone surrounded by a peripheral, erythematous halo. Cutaneous EM starts on the extremities and may spread centripetally. It appears within 24 hours of being triggered and fully evolves by 72 hours. It is usually asymptomatic, but occasionally patients experience pruritus and a burning sensation.
EM can be subclassified as minor or major depending on whether mucous membranes are involved.1 Prodromal symptoms such as fever and malaise are more commonly seen in EM major.5 The diagnosis is clinical; skin biopsy usually shows nonspecific changes. EM generally resolves in 3 to 5 weeks. Postinflammatory pigment alternations may occur in some cases and last for several months.5 Occasionally, corticosteroids and antihistamines are administered to reduce symptoms.
We were later informed that the local county’s vector control unit had been spraying phenothrin. Phenothrin is low in toxicity when exposed to skin and eyes; however, it can cause mild skin sensitivity, including itchy tingling and burning. This symptom usually subsides within 48 hours. The Environmental Protection Agency has determined that phenothrin is not carcinogenic. The half-life is 38 to 72 minutes in the air. Animal studies have not indicated a carcinogenic property.6
The EM rash presented in an almost identical fashion among all 3 patients—the distribution, morphology, presence of fever, disease course, elevation of ESR, estimated body surface area, location, and minimal mucosal involvement. No medical conditions predisposed the patients to EM; the only shared exposure was phenothrin. Therefore, we suspect that the pesticide was the precipitator of the cases of EM minor.
The differential diagnosis of EM includes irritant contact dermatitis.7 However, the presence of fever, the appearance of skin lesions on sun-protected sites, the lack of significant pruritus, and the absence of eosinophils on histology testing argued against this diagnosis. Additionally, urticaria multiforme lesions usually fade away in 24 hours, Steven-Johnson syndrome commonly involves the mucosa and is triggered by drugs, and Rocky Mountain spotted fever typically presents with petechiae and headache. Skin biopsy was performed in our patients to rule out vasculitis and bullous diseases.1
To our knowledge, EM secondary to phenothrin exposure has not been previously reported. In one case report, an EM-like eruption due to irritant contact dermatitis from a glyphosate pesticide was documented.7
In conclusion, pesticides may be a trigger of EM minor. The condition self-limited, without significant involvement of mucosal surfaces. However, further studies are warranted to monitor for recurrence and possible long-term sequelae.
REFERENCES:
- Wetter DA. Erythema multiforme: pathogenesis, clinical features, and diagnosis. UpToDate. https://www.uptodate.com/contents/erythema-multiforme-pathogenesis-clinical-features-and-diagnosis. Updated February 15, 2019. Accessed December 9, 2019.
- Lamoreux MR, Sternbach MR, Hsu WT. Erythema multiforme. Am Fam Physician. 2006;74(11):1883-1888.
- Athanasiadis GI, Pfab F, Klein A, Braun-Falco M, Ring J, Ollert M. Erythema multiforme due to contact with laurel oil. Contact Dermatitis. 2007;57(2):116-118. doi:10.1111/j.1600-0536.2006.00869.x
- Kushner T, Shinkai K, Fox L, et al. New presentation of autoimmune hepatitis with erythema multiforme. Hepatology. 2018;67(4):1628-1630. doi:10.1002/hep.29610
- Sokumbi O, Wetter DA. Clinical features, diagnosis, and treatment of erythema multiforme: a review for the practicing dermatologist. Int J Dermatol. 2012;51(8):889-902. doi:10.1111/j.1365-4632.2011.05348.x
- d-Phenothrin general fact sheet. National Pesticide Information Center. http://npic.orst.edu/factsheets/dphengen.html. Reviewed December 2011. Accessed December 9, 2019.
- Heras-Mendaza F, Casado-Fariñas I, Paredes-Gascón M, Conde-Salazar L. Erythema multiforme-like eruption due to an irritant contact dermatitis from a glyphosate pesticide. Contact Dermatitis. 2008;59(1):54-56. doi:10.1111/j.1600-0536.20001307