
Angiosarcoma of the Small Intestine With Metastases to the Colon and Gallbladder
An 81-year-old man with a history of hypertension, type 2 diabetes mellitus, and Alzheimer disease presented with syncope. The patient denied having chest pain, dyspnea, palpitations, nausea, vomiting, hematochezia, melena, facial droop, slurred speech, or a history of seizure. He did not use aspirin or nonsteroidal anti-inflammatory drugs.
Physical examination. The patient’s vital signs were stable. He had dry mucosal membranes, diffuse abdominal pain on palpation, hypoactive bowel sounds, and pale skin with poor skin turgor.
Diagnostic tests. Fecal occult blood test (FOBT) results were positive. Laboratory test results were significant for the following values: hemoglobin, 5.6 g/dL (reference range, 14-18 g/dL); hematocrit, 18.8% (reference range, 42%-52%); serum iron, 14 µg/dL (reference range, 65-175 µg/dL); total iron binding capacity, 184 µg/dL (reference range, 280-400 µg/dL); and iron saturation, 8% (reference range, 20%-50%).
The patient underwent upper and lower gastrointestinal (GI) endoscopic examination due to a suspected GI tract bleed based on the positive FOBT results. The upper endoscopy findings were normal. Colonoscopy, however, revealed a 1-cm flat ulcerated area in the mid-ascending colon, which was biopsied.
In light of the patient’s report of diffuse abdominal pain on physical examination, computed tomography (CT) scanning of the abdomen and pelvis was performed, the results of which demonstrated intussusception of a loop of the jejunum (Figures 1A and 1B).

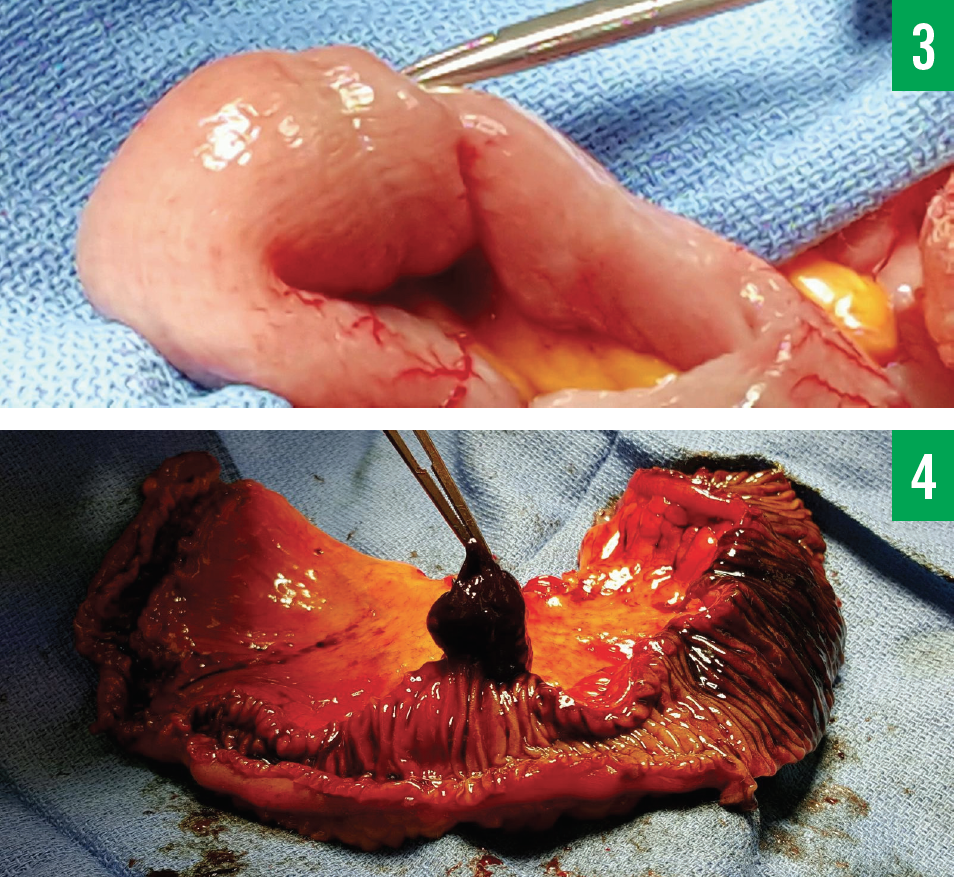
The patient then underwent an exploratory laparotomy, during which 2 areas of small bowel intussusception were found and excised (Figures 2-4). The first area of intussusception was at the level of the mid-jejunum and contained a 1.8 × 1.3-cm lesion. The second area was in the terminal ileum and contained a 2.5 × 2.0-cm lesion.
The small bowel lesions, along with the colon and gallbladder biopsy specimens, were examined histologically and immunohistochemically. Neoplasms were found in all 4 specimens. Sections from these lesions showed a very pleomorphic epithelioid neoplasm. There was an extensive vascular invasion, and in some foci, the atypical cells appeared to be lining vessels.
A diagnosis of primary angiosarcoma of the small intestine with metastases to the right colon and gallbladder was made.
Treatment. The patient underwent an exploratory laparotomy to remove the small bowel lesions, which had been causing the acute blood-loss anemia that had led to the patient’s syncope. He also underwent a cholecystectomy for chronic cholecystitis, the placement of gastrostomy tube, and a right hemicolectomy.
He received multiple blood transfusions to maintain stable hemoglobin and hematocrit levels. He was placed on total parenteral nutrition and then advanced to tube feeding.
Discussion. Angiosarcomas are rare malignant vascular tumors that account for 1% to 2% of all sarcomas.1,2 Intestinal angiosarcoma is extremely rare, with fewer than 30 cases of intestinal angiosarcoma published in the literature.1
The list of differential diagnoses includes adenocarcinoma, neuroendocrine tumor, malignant melanoma, Crohn disease, GI stromal tumor, lymphoma, intestinal tuberculosis, leiomyosarcoma, and fibrosarcoma.
Intestinal angiosarcoma typically presents with GI bleeding, fatigue, anemia, weakness, abdominal pain, intestinal obstruction, abdominal distention, and weight loss.3,4 The pathogenesis of intestinal angiosarcoma is unknown. Angiosarcoma has been associated with prior radiation exposure, chronic lymphedema (Stewart-Treves syndrome), exogenous toxins (eg, vinyl chloride, thorium dioxide, arsenic, anabolic steroids, foreign bodies), and familial syndromes (eg, neurofibromatosis type 1, BRCA1 and BRCA2 mutations, Maffucci syndrome, Klippel-Trénaunay syndrome).1,5
Tests that can aid in making the angiosarcoma diagnosis include radiography, ultrasonography, CT, positron emission tomography, and magnetic resonance imaging.6 The lesions and sources of bleeding can be detected with the use of endoscopy, exploratory laparoscopy, and laparotomy. Results of pathologic and immunohistochemical examinations can contribute to the definitive diagnosis of angiosarcomas.5
Staging of soft tissue sarcomas is with the TNMG system, which uses tumor size (T) and depth (superficial or deep), lymph node involvement (N), the presence or absence of distant metastases (M), and histologic grade (G) in determining the stage.
Surgery is the primary treatment approach for angiosarcoma. Chemotherapy and/or radiation therapy may be administered before or after surgery. The chemotherapy of choice for angiosarcomas has been taxanes (paclitaxel or docetaxel), doxorubicin, or pegylated liposomal doxorubicin.7,8
Outcome of the case. After surgery, the patient received postoperative care and rehabilitation. Given the patient’s advanced Alzheimer disease and age, supportive care was determined to be most beneficial management approach. The patient was discharged to a skilled nursing facility.
Vinh-Quang Do Nguyen, DO, is an internist at Corpus Christi Medical Center–Bay Area in Corpus Christi, Texas.
Aftab Mahmood, MD, is a hematologist at Cancer Specialists of South Texas in Corpus Christi, Texas.
Michael Caberto, DO, is an internist at Corpus Christi Medical Center–Bay Area in Corpus Christi, Texas.
REFERENCES:
- Ni Q, Shang D, Peng H, et al. Primary angiosarcoma of the small intestine with metastasis to the liver: a case report and review of the literature. World J Surg Oncol. 2013;11:242.
- Brennan MF, Alektiar KM, Maki RG. Soft tissue sarcoma. In: DeVita VT Jr, Hellman S, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:1841-1891.
- Mohammed A, Aliyu HO, Liman AA, Abdullahi K, Abubakar N. Angiosarcoma of the small intestine. Ann Afr Med. 2011;10(3):246-248.
- Allison KH, Yoder BJ, Bronner MP, Goldblum JR, Rubin BP. Angiosarcoma involving the gastrointestinal tract: a series of primary and metastatic cases. Am J Surg Pathol. 2004;28(3):298-307.
- Khalil MF, Thomas A, Aassad A, Rubin M, Taub RN. Epithelioid angiosarcoma of the small intestine after occupational exposure to radiation and polyvinyl chloride: a case report and review of literature. Sarcoma. 2005;9(3-4):161-164.
- Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ. Angiosarcoma. Lancet Oncol. 2010;11(10):983-991.
- Fury MG, Antonescu CR, Van Zee KJ, Brennan MF, Maki RG. A 14-year retrospective review of angiosarcoma: clinical characteristics, prognostic factors, and treatment outcomes with surgery and chemotherapy. Cancer J. 2005;11(3):241-247.
- Young RJ, Natukunda A, Litière S, Woll PJ, Wardelmann E, van der Graaf WTA. First-line anthracycline-based chemotherapy for angiosarcoma and other soft tissue sarcoma subtypes: pooled analysis of eleven European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group trials. Eur J Cancer. 2014;50(18):3178-3186.