
Peer Reviewed
Acute Pericarditis
Authors:
Sudhir R. Gogu, DO, PhD, MBA
Clinical Assistant Professor, Texas Tech University Health Sciences Center, Lubbock/University of Texas Health Science Center at San Antonio/University of North Texas Health Science Center, Fort Worth/University of the Incarnate Word School of Osteopathic Medicine, San Antonio, Texas; and Stone Oak Urgent Care and Family Practice, San Antonio, Texas
Swetha Gogu, BS, OMS-II
Osteopathic Medical Student, Kansas City University of Medicine and Biosciences, Kansas City, Missouri
The parents of a 17-year-old boy sought medical care for their son after he reported having had intermittent chest pain for 3 days.
Physical examination. The patient denied shortness of breath, radiating pain, nausea, fever, and chills. He described the pain as 8 of 10 while standing, bending, coughing, or running and 3 of 10 at rest. His vital signs were stable; there was no clubbing, cyanosis, murmur, or gallop. However, a mild pericardial friction rub was noted. The pain increased with palpation of the left upper quadrant. Examination findings of the lungs, abdomen, and extremities were normal, and the patient was neurologically intact.
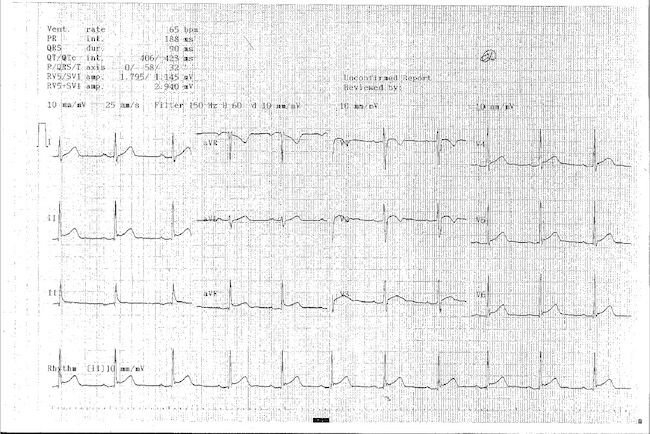
Diagnostic tests. Results of a complete blood cell count and a comprehensive metabolic profile were within normal limits. An electrocardiogram (ECG) showed significant ST elevation in chest lead II (Figure) and limb leads V3, V4, and V5. The patient’s heart rate was normal at 60 beats/min. Other laboratory test results and radiography findings were within normal limits, suggesting that the patient had acute pericarditis.
Discussion. Acute pericarditis is an inflammation of the pericardium. It is often characterized by chest pain, pericardial friction/rub, serial ECG changes (new ST elevation or PR depression), and pericardial effusion. Supportive findings for the diagnosis of acute pericarditis include elevation in the white blood cell count, the erythrocyte sedimentation rate, and the C-reactive protein level, as well as evidence of inflammation on imaging results. A variety of infectious and noninfectious processes can cause pericarditis; however, the idiopathic and viral forms are the most common.1
Acute pericarditis is self-limiting in most patients. A treatment course consisting of bed rest, nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, and corticosteroids may relieve the pain of patients with viral or idiopathic acute pericarditis. However, when the identified etiology is not viral or idiopathic, management should be directed toward treating the underlying cause.2
Outcome of the case: A 1-week course of NSAIDs relieved our patient’s symptoms.
References:
- Xanthopoulos A, Skoularigis J. Diagnosis of acute pericarditis. E J Cardiol Pract. 2017;15(15). https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-15/Diagnosis-of-acute-pericarditis. Accessed July 19, 2018.
- Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010;85(6):572-593.