
Aspiration Pneumonia as a Harbinger of Squamous Cell Carcinoma of the Larynx
Case In Point
An Intriguing Diagnosis
 A 48-year-old woman with a 50-pack year smoking history presented with worsening dyspnea and progressive weight loss of 25 lb over the previous 4 months. In addition, she had a productive cough with yellowish-brown sputum during the past few weeks, which was not associated with fever, chills, hemoptysis, or night sweats. She also reported halitosis, dysphagia, and hoarseness.
A 48-year-old woman with a 50-pack year smoking history presented with worsening dyspnea and progressive weight loss of 25 lb over the previous 4 months. In addition, she had a productive cough with yellowish-brown sputum during the past few weeks, which was not associated with fever, chills, hemoptysis, or night sweats. She also reported halitosis, dysphagia, and hoarseness.
Physical examination of the oropharynx did not reveal any obvious abnormalities other than poor dentition and halitosis. Other findings were bitemporal wasting, cachexia, and scattered apical crackles. A chest radiograph (Figure 1) suggested bilateral cavitary lesions. A CT scan of the chest (Figure 2) showed left hilar adenopathy and multiple bilateral cavitary lesions with thickened and irregular walls, as well as dense consolidation in the lingular segment of the left upper lung consistent with an inflammatory process. The differential diagnosis initially included septic embolization, pulmonary tuberculosis, Wegener granulomatosis, and fungal infection.
 An acid-fast bacillus smear was negative. The C-reactive protein level was elevated at 40.9 mg/L. Tests for CH50, anti-GBM AB, PPD, C-ANCA, P-ANCA, C3, C4, and ANA were negative. An echocardiogram was normal.
An acid-fast bacillus smear was negative. The C-reactive protein level was elevated at 40.9 mg/L. Tests for CH50, anti-GBM AB, PPD, C-ANCA, P-ANCA, C3, C4, and ANA were negative. An echocardiogram was normal.
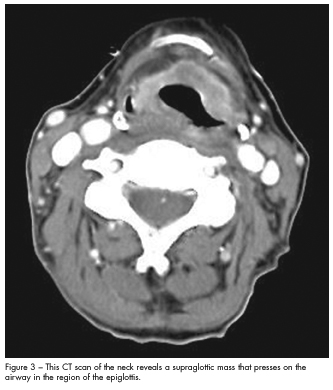
Because of her dysphagia, a videofluoroscopic swallow study was done, which suggested aspiration. This prompted a triple endoscopy that revealed an exophytic mass on the epiglottis along with right vocal cord paralysis. A CT scan of the neck (Figure 3) showed a supraglottic mass that impressed on the airway in the region of the epiglottis. CT-guided fine needle aspiration of the cavitary lesion revealed pulmonary epithelial cells, histiocytes, and muscle fibers suggestive of aspiration. There were no malignant cells.
A diagnosis of supraglottic squamous cell carcinoma stage T4aN0Mx complicated by bilateral cavitary aspiration pneumonia was made. The patient was treated with ampicillin/sulbactam to which she responded well, and she had a tracheostomy followed by a percutaneous endoscopic gastrostomy. A PET scan was scheduled prior to the initiation of radiation therapy.
 CASE DISCUSSION
CASE DISCUSSION
Aspiration pneumonia following the treatment of squamous cell carcinoma of the larynx is well described. Its prevalence is high after supracricoid hemilaryngopharyngectomy because of resection of the ipsilateral superior laryngeal nerve.1 In addition, a retrospective study of patients who presented with dysphagia after concurrent chemoradiation for head and neck cancers demonstrated a high prevalence of aspiration.2 However, it is uncommon for aspiration pneumonia to precede the diagnosis of squamous cell carcinoma, as it did in this patient.
Diagnosis. Patients with hypopharyngeal or laryngeal cancers generally present with chronic inflammatory changes of the pharynx caused by smoking, often leading to a diagnosis of chronic pharyngitis. Referred otalgia may also be a presenting symptom. Twenty percent of patients with hypopharyngeal cancer present with an asymptomatic neck mass. Almost all cancers of the hypopharynx are squamous cell carcinomas, and the vast majority of patients present with at least stage III disease. Laryngeal cancer is 3 times as common as hypopharyngeal cancer and often is detected earlier because affected patients complain of hoarseness.3
Etiology. Men are more susceptible than women to cancer of the hypopharynx; however, certain women of Scandinavian descent have an increased incidence of hypopharyngeal cancer as well as Plummer-Vinson syndrome. Tobacco and ethanol are the principal carcinogens responsible. Inheritable polymorphisms of expression of enzymes that activate proto-carcinogens (eg, aryl hydrocarbon hydroxylase) and detoxify carcinogens (eg, glutathione S-transferase) have been identified.4
Treatment. Standard treatment options include total laryngectomy with postoperative radiation therapy and definitive radiation therapy with surgery for salvage of radiation failures. Consider chemotherapy administered concomitantly with radiation therapy for patients who would require total laryngectomy for control of disease; reserve laryngectomy for patients who have a less than 50% response to chemotherapy or who have persistent disease following radiation.5 T1-T2 tumors show similar outcomes with radiation or surgery.
Surgery can be coupled with radiation and, possibly, chemotherapy in more advanced cancers (T3-T4, N-positive). The extent of surgery for primary tumors depends on the local extent. Patients treated for laryngeal cancers are at highest risk for recurrence in the first 2 to
3 years. Recurrences after 5 years are rare and usually represent new primary malignancies. Close, regular follow-up is crucial to maximize the likelihood of salvage.
Newer treatment options under evaluation include hyperfractionated radiation therapy and isotretinoin (ie, 13-cis-retinoic acid).6,7 ■
1. Laccourreye H, Lacau St Guily J, Brasnu D, et al. Supracricoid hemilaryngopharyngectomy. Analysis of 240 cases. Ann Otol Rhinol Laryngol. 1987;96(2 Pt 1):217-221.
2. Nguyen NP, Moltz CC, Frank C, et al. Dysphagia following chemoradiation for locally advanced head and neck cancer. Ann Oncol. 2004;15:383-388.
3. Schreiner C, Quinn FB Jr. Hypopharyngeal cancer. University of Texas Medical Branch at Galveston Department of Otolaryngology Grand Rounds; March 5, 1997.
4. Quon H. Hypopharyngeal cancer. Emedicine. http://emedicine.medscape.com/article/1375268. Accessed August 16, 2011.
5. Adelstein DJ, Lavertu P, Saxton JP, et al. Mature results of a phase III randomized trial comparing concurrent chemoradiotherapy with radiation therapy alone in patients with stage III and IV squamous cell carcinoma of the head and neck. Cancer. 2000;88:876-883.
6. Hong WK, Lippman SM, Itri LM, et al. Prevention of second primary tumors with isotretinoin in squamous-cell carcinoma of the head and neck. N Engl J Med. 1990;323:795-801.
7. Laryngeal cancer treatment. National Cancer Institute Web site. http://www.cancer.gov/cancertopics/pdq/treatment/laryngeal/HealthProfessional/page6. Accessed August 16, 2011.